
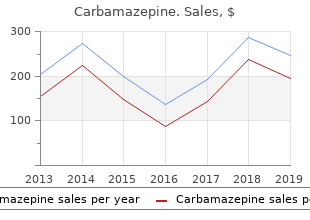
Union College, Barbourville KY. X. Frithjof, MD: "Order Carbamazepine online - Safe Carbamazepine".
When you 12 Micro-organisms are found identify the hazard purchase generic carbamazepine from india muscle relaxant homeopathic, you need to find virtually everywhere in the natural out about the links in the chain to help environment order online carbamazepine muscle relaxant id. Most of these are you identify the best way to break it harmless to humans and do many and so control the risk buy carbamazepine 200mg line spasms in your back. Host Bacteria live on or in just Source about every material and environment, from soil to Sources water to air, and from the deep ocean to Arctic ice to 17 There are four main sources of volcanic vents. There are infection that you need to consider in more bacterial cells in the a workplace: human body than there are human cells, and some are ? blood and other body fluids (eg saliva) and sources of absolutely necessary to our blood/body fluids such as human survival. On each square bodies, animal carcases and raw centimetre of our skin there meat; are about 100 000 bacteria and a single teaspoon of ? human or animal waste products topsoil contains more than a such as faeces, urine and vomit; billion bacteria. The cells of these linings and the Transmission substances they produce are the A tattooist sterilises needles to remove body�s first line of defence. If a micro- infectious micro- 19 To become infected, the micro- organism does manage to cross this organisms that might organism has to get from the source barrier, the next line of defence is the be present in blood, into the host by some means. The outward signs and symptoms of disease such as fevers 20 Infection at work can occur via: or rashes are a result of this contest. You ? breathing in infectious should check this before employees aerosols/droplets from the air, start work, so you can make sure they eg respiratory discharges such are protected or give them less as coughs and sneezes, hazardous work to do. This is not an exhaustive A cleaner of public with infectious micro-organisms at list, but it does include the most toilets wears protective work. This may be as a result of commonly occurring occupationally gloves and washes their contact with people or animals, or else acquired infections. Other micro- hands when finished to your workplace itself may be a source organisms may create a risk, so prevent infectious of contamination. For example legionella bacteria are equally at home in cooling towers or deadlegs of hot and cold water services as they are in the natural aquatic environment. When you have identified the source(s) of infection, you need to consider how likely it is that infection will result - think about: ? how often the task is carried out; ? how many employees are exposed; and ? how much infectious material is handled. Appendix 1 to record your assessment, or you could include infection hazards in your general workplace risk assessment. When considering direct contact with people or animals, you need to address risks from the living and the dead, as well as risks from handling material such as raw meat. You have a duty under health and safety law to consult with employees about health and safety matters. As well as giving employees information, you need to listen and take account of what they say before making any health and safety decisions. Ask your employees if they have come across any hazards you haven�t identified, eg areas where dirty/used needles might be dumped. Make sure you identify all those who might be affected, not just employees � remember contractors, members of the public and others. There may be animals, including insects, in your workplace that you cannot see or that you have no direct control over: pests such as rats, pigeons, cockroaches, ticks etc. If your work involves people or animals, they may appear healthy, because infection may not be associated with obvious signs. These measures should be 32 Once you have carried out your applied in all workplaces. You should consider, if you basis to keep the equipment you can: use and the workplace clean. This means controlling exposure, ie the risk of infection, to a level that won�t harm people�s health. However, you need to remember that, unlike some chemicals, there are no exposure limits for micro-organisms. And your control measures need to take into account the fact that: ? micro-organisms can grow and multiply; and ? infection could be caused by exposure to only a few micro- organisms. There are two main approaches that you should use for the control of infection: ? for work with people or animals, the basic control principles of good occupational hygiene should be applied in all situations (Checklist 1). You may also need to supplement these measures with other controls depending on the work activity (as shown in the supplementary controls list); and ? the principles of good environmental hygiene and design (Checklist 2) to stop or. If cuts and grazes occur, wash immediately with soap and running water and apply a waterproof dressing. Supplementary controls ? If the work activity could result in a skin piercing/cutting injury, the risk of puncture wounds, cuts or grazes should be controlled by avoiding the use of sharp objects, eg needles, glass, metal, knives etc. If this is not possible, safe working practices for handling and disposal of sharps should be used and appropriate protective equipment provided. If this is not possible, appropriate respiratory protective equipment should be used. You need to wash your hands: before: ? you eat, drink, take medicine, put on make-up, insert contact lenses etc; and after: ? any work activity where you may have become contaminated. How to wash your hands You may think you know but you should: ? use soap and warm, running water; ? wash all surfaces thoroughly, including wrists, palms, back of hands, fingers and thumbs and under the fingernails; ? rub hands together for at least 10-15 seconds; ? rinse and dry hands - if towels are used, these should be clean or disposable. But if staff have to wash it themselves, it should be washed at the highest temperature possible and separately from other uncontaminated clothing. As well as controlling the risks on a day-to day basis, you also need to consider what you would do in an emergency situation. For example if an employee suffered a skin-penetrating injury from a blood-contaminated sharp. Most micro-organisms will be physically removed and/or killed if you clean your work surfaces/areas with hot water and detergent. If you chose to use a disinfectant, eg bleach, you need to make sure that it kills the micro- organisms that you want killed and that it doesn�t damage your work surfaces/areas - or cause any health problems for your employees. You also need to make sure that the process of cleaning doesn�t create any risk, eg use low pressure hosing for cleaning large areas to avoid creating infectious aerosols. If your employees don�t have direct access to warm running water to wash their hands, for example because they aren�t based at any one location, you may be able provide a suitably designed vehicle with facilities on board. Alternatively, you may provide alternatives such as antiseptic wipes or hand cleansers. For control measures to work, you need to tell your employees about the risks that you have identified and the measures you have put in place to control exposure. They need to know and understand when and how to apply the controls, including the use of personal protective equipment; and what to do in an emergency. You may decide to tell your employees this information or else it may form part of their job instructions/the local code of practice or standard operating procedure. Make sure you let anybody else who might be at risk know about the controls too, eg members of the public. Consider whether hazard can be eliminated List those who are at risk from sources of infection here List control measures here Further information. Example assessments Name of organisation Gosford Borough Council � Environmental Services Department Name of assessor W McCordle Date of assessment 1/1/03 General description Park/open space maintenance of work Specific activity Collection and disposal of litter from parks and other council assessed - maintained open spaces, eg playing fields List source(s) of Contact with contaminated sharp objects in the form of discarded infection here. Happens at least once a week, can be up to 20 needles in some places Consider whether hazard can be Not possible to eliminate the hazards, there are sharps bins in the eliminated public toilets in the parks, but these are not always used List those who are All park-keepers/groundsmen at risk from sources of infection here List control measures Use rubbish picker or dustpan and brush to remove rubbish.
Diseases
The incidence of neurocognitive sequelae Lactic acidosis commonly coexists with hypoglycemia and is following severe malaria is only a fraction of the true residual (with coma buy generic carbamazepine 200mg line muscle relaxant chlorzoxazone side effects, repeated convulsions buy carbamazepine no prescription muscle relaxant mechanism, shock purchase 100mg carbamazepine muscle relaxant agents, and hyperpara- burden, and the impact of milder illness is unknown. Some considerably depending on the background spectrum of other consider anemia to be caused indirectly unless linked to acute, common diseases, such as acute respiratory infection, gas- high-density parasitemia. Similarly, low birthweight may also troenteritis, and meningitis, which share common clinical be indirectly attributable to malaria, and a child�s later under- features with malaria (Korenromp and others 2003). Thus, households will detect a quarter of the medical events that are malaria infection contributes to broad causes of mortality detected through weekly surveillance, and weekly contacts with beyond the direct fatal consequences of infection and is prob- cohorts identify approximately 75 percent of events detected ably underestimated (Breman, Alilio, and Mills 2004; Snow through daily surveillance (Snow, Menon, and Greenwood and others 2003). Given the predominance of fevers, malaria case man- In Africa, pregnant women experience few malaria-specific agement in Africa and other endemic areas usually centers on fever episodes but have an increased risk of anemia and presumptive diagnosis. Maternal clinical mani- Estimates of the frequency of fever among children suggest festations are more apparent in areas with less intense one episode every 40 days. Estimates indicate that in frequency of fever in Africa is similar across all transmission Sub-Saharan Africa, malaria-associated anemia is responsible areas (and possibly all ages), African countries would witness for 3. Assuming an infant mortality rate of 105 and drug delivery assumptions are debatable, they indicate the per 1,000 live births, Snow and others (2003) calculate that in magnitude of the challenges malaria presents. Murphy and Breman (2001) report a mean case- malaria-associated low birthweight accounted for 62,000 to fatality rate of 19. Those who succumb at home without Anemia among African children is caused by a combination optimal treatment will have higher case-fatality rates. Reducing the incidence of new infec- and Breman 2004; Schellenberg and others 2005). Eliminating undernutrition is its congruence with the distribution of malaria from most endemic areas remains a distant, huge, but endemic malaria. Indeed, Brazil, Eritrea, India, and Vietnam are reporting infection approximately doubles the risk of malaria parasitemia recent successes in reducing the malaria burden (Barat 2005). Yet, treatment of patients lends credibility to the malaria program, evaluation of trimethoprim-sulfamethoxazole for malaria pro- strengthens confidence in the health care system by families phylaxis in Mali did not show any increases in parasite resistance and communities, and raises the esprit of clinicians and public mutations specific for these drugs (Thera and others 2005). Malaria accounts for 13 to 15 percent of medical reasons for absenteeism from school, but little information is available on Early Diagnosis and Treatment. Early diagnosis and effective the performance of parasitized schoolchildren (Holding and treatment can cure infection, prevent further morbidity Kitsao-Wekulo 2004). A randomized placebo control study of and progression to severe disease and death, and arrest chloroquine prophylaxis in Sri Lankan schoolchildren demon- transmission. This intervention requires timely and accurate strated an improvement in mathematics and language scores diagnosis; use of efficacious drugs; education of patients and by those who received chloroquine but found no difference in their families about the disease, home management, and 418 | Disease Control Priorities in Developing Countries | Joel G. The following targets for specific intervention strategies were established at the Abuja Malaria Summit in April 2000. Strategy Abuja target (by 2005) � Prompt access to effective treatment � 60 percent of those suffering with malaria should have access to and be able to use correct, affordable, and appropriate treatment within 24 hours of the onset of symptoms. A febrile malaria attack warrants early treat- cost-effectiveness of this new strategy is needed (Arrow, ment. Effective management of sis of malaria is based on detection of the parasite and, if patients requires skilled and well-equipped personnel at all laboratory diagnosis is not feasible, on clinical grounds. The two strategies for delivering Health workers must monitor the therapeutic efficacy of antimalarials effectively are through health facilities and in drugs closely and change treatment policies when parasite or near the home when access to health facilities is limited. The box indicates the 25th�75th percentile, the vertical line the lower and upper values, and where the lines cross the median. Chemoprophylaxis is advised by travel implemented in conjunction with enhanced vector control; medicine specialists for nonresidents of endemic areas who are thus, effective treatment alone does not account for the fall in exposed to malaria for short periods. The choice of chemoprophylaxis will depend on the the impact of early and effective treatment on malaria trans- drug-sensitivity profile, tolerance, side effects, costs, regimen, mission. Studies in 37 countries indicate the need for a doses during vaccination or well-baby visits to health clinics. Many countries are also trying to show that Eritrea, Malawi, Togo, Zambia, and other countries improve the time lag before treatment. More than 83 percent of in Africa are already scaling up nationally with high coverage. In Burkina Faso, Ethiopia, and Uganda, where access tothe reduction of Anopheles breeding and biting of humans clinics was poor and difficult, mothers and community health involves different methods of insecticide and repellent applica- workers were empowered to dispense treatment, which result- tion, environmental management, and behavioral change of ed in major reductions in mortality and morbidity in children populations at risk. Examples of successful and sustained malaria elimina- in both stable and unstable transmission areas. Larviciding is the application of lasting insecticidal property are now available, and re- chemical insecticides, including those of biological origin and treatment will soon cease to be an issue. Fogging or space spraying Conquering Malaria | 421 with insecticides requires specialized equipment, because the These persons are an extension of the health system and work particle size of the insecticide determines its suspension quali- under the direct supervision of health facility staff or non- ties in the air, the number of droplets, and the penetration of governmental organizations and in conformity with standards space. Such information can help to increase the standard of target mosquito activity, generally at night. They find that in a very low-income country, the cost-effectiveness range Civil Engineering. Goodman, Coleman, and Mills (2000) find that globally, and at development project sites where earth removal even though some interventions are relatively cheap, achieving has occurred. Commercially available mosquito repellents are applied directly on the skin or clothing as aerosols, lotions, or creams and Analysis contain active ingredients that protect the individual from mos- quito bites. Commercially available mosquito coils containingthe following analysis incorporates new knowledge on the pyrethroids can be burnt to repel mosquitoes, and electrically effects of interventions and on their costs for a low-income, heated dispensers serve a similar function. Some communities Sub-Saharan African population living in an area of high, in endemic regions use smoke, burning herbs, or plants to deter stable transmission. The approach used and effective ingredient in commercially available repel- allows for changing cost-effectiveness over time, for example, as lents (Curtis and others 1991). While several studies have shown resistance to antimalarial drugs or insecticides increases. We assumed that cost Health Education and Counseling and effectiveness input variables follow uniform triangular or Health education is the provision of information via news- normal continuous probability distributions (Mulligan, Morel, papers, radio, or television, and health counseling is interactive, and Mills 2005). We include tance of early treatment and where to access it, the use of costs to the provider and the community and incremental out- referral services, and the significance of full compliance with of-pocket expenses for households, but because of major treatment and other interventions. The necessary information valuation and measurement problems, we do not include the can be provided by community and voluntary health workers. These results should be interpreted with caution costs for all interventions except patient management, given because of uncertainty in relation to the estimates of effective- the uncertainty inherent in estimating savings. The model was based on one round of spraying per year in areas of seasonal transmission and two Insecticide-Treated Nets. In relation to malathion and deltamethrin for only two to three months insecticide, we considered permethrin and deltamethrin. We analyzed benefits to the child staff and community health workers, a campaign to inform the by decreased mortality and benefits to the mother resulting community about the intervention, the procurement and from changes in the incidence of severe anemia. We calculated cost- increased birthweight based on the Cochrane meta-analysis effectiveness for each intervention for two scenarios: one of malaria prevention in pregnancy (Gulmezoglu and Garner whereby nets were distributed to households and the second 1998). The model allowed for level of drug resistance, prob- whereby treatment was arranged for existing nets.
Discount carbamazepine 400 mg with amex. Natural Muscle Relaxation Teas for Anyone Suffering From Muscle Spasms or Other Muscular Ailments.
Patients (any age); 2007 � decisionmaking buy carbamazepine mastercard spasms after hemorrhoidectomy, shared Quality of decision buy 100 mg carbamazepine free shipping muscle relaxant drugs flexeril, mean score (1?10): acute respiratory March 2008 decisionmaking support tools buy genuine carbamazepine on line muscle relaxant tl 177. Intention to engage in shared decisionmaking, mean score (?3 to +3): Clinicians: 0. Intention of clinicians to comply with clinical practice guidelines, mean score (?3 to +3): ?0. Other Point-of-Care Tests (Procalcitonin, Viral, Rapid Strep) No evidence was found for other point-of-care tests. What are the comparative nonclinical adverse effects of strategies for improving the appropriate use of antibiotics for acute respiratory tract infections (e. Key Points � Evidence was insufficient to draw conclusions about the nonclinical adverse effects of interventions to improve appropriate antibiotic prescribing. There are no estimates on the time and other resources needed to develop and deploy the interventions within a clinic or health system. A few studies described the amount of time interventions required of the participants, but very few addressed the time needed for development of the educational materials. Of the studies reporting the time required for clinicians participating in 61,73,84,99,106,131,148 educational sessions, seven were 1 to 5 hours in duration and two were 1 and 2- 114,166 day sessions. There was no assessment of whether or when such sessions might need to be repeated. Video 47,118,124,176 interventions lasted 3 to 20 minutes depending on whether they were intended to be viewed in the clinic or at home. Time required for reading educational pamphlets were reported 118,150 only in two studies, reported as 5 to 15 minutes. An interactive computer kiosk educational program took patients 9 to 45 minutes complete. Finally, child care workers were given 45- minute presentations but the time each of these participants spent subsequently educating parents 66,148 was not recorded. Communication Interventions None of the seven trials of interventions to improve communication between clinicians and patients explicitly measured adverse consequences of creating and implementing the intervention, although some discussed related issues such as lack of participation by some clinicians. Six trials described the amount of time the various interventions required of the 41,51,56,86,87,95 participants. Five of the trials targeted clinicians, four of which had interventions 51,56,86,87 requiring between 4 hours and 10 hours of participant time: � Combined communication and educational intervention about prescribing guidelines 51 required a combined total of 10 hours. In contrast, a trial using an internet-based training module reported a mean time of 37. The single trial that targeted the parents of pediatric patients 41 required seven minutes of participant time. Although these are real concerns for the feasibility of such communication training interventions, at least one trial recognized the potential counter-balancing benefit of providing 87 continuing medical education credit for participating clinicians. Another trial found that the effect of communication training on antibiotic prescribing may extend for several years, suggesting that a long-term benefit of such interventions may counter balance the time required 57 56 up front. Conversely, the single poor-quality trial found that the rate of antibiotic prescription among clinicians who received communication training, which decreased at 6 weeks after the intervention (from 36. Clinical Interventions Delayed Prescribing Strategiesthe studies of clinical strategies did not specifically measure or report on increased time burden on clinicians, sustainability of intervention (e. Compared with issuing an immediate antibiotic prescription, conceivably there is at least some increase in time burden for clinicians using delayed prescribing strategies in (1) getting oriented to using a new prescribing approach, (2) explaining to patients the likely natural history of their illness and that it would probably not be helped by antibiotics, (3) providing instructions on how to decide if and when to use the prescription, and (4) fielding patients� related questions. For example, one study provided the standardized script that clinicians were asked to use when issuing a delayed prescription, which was 235 words in length and would likely require a few minutes to read to their 133 patients. Delayed antibiotic prescription strategies requiring recontact would also require increased time for clinicians and patients compared with immediate antibiotics or delayed antibiotic strategies in which the prescription was given at the time of the visit with instructions 92 to delay or with postdating. Delayed strategies requiring the patient to return for collection of 92 the prescription would also require more patient time. For standardized decision rules, although there would likely be an initial time investment for clinicians in getting oriented to its use, how the time burden of its implementation would compare to that of the usual care process of deciding whether immediate antibiotics are needed would likely vary based on the complexity of the decision rule. For example, the sore throat decision rule utilized in the single relevant study we identified, was very simple, only including scoring of four objective indicators (e. Four trials described the amount of 56,58,80,95 time the various interventions required of the participants. One trial used an intervention with an internet-based training module (mean time 26. Procalcitonin Point-of-Care Testingthe five trials and two reviews of procalcitonin did not specifically measure or report on increased time burden on clinicians, sustainability of intervention (e. The studies reported a range of 1 to 4 hours for test results being reported to the clinician, depending on where and how it was processed and reported. In all studies, clinicians communicated with patients via telephone to provide instructions on antibiotic use following interpretation of the test result. In some the patients had all been given a prescription and asked to not fill it until they heard from the clinician. Those who were deemed to not need an antibiotic were asked to return the prescription by mail. While these procedures may have been study related, they do raise questions about what process is used for handling prescribing decisions when the decision is delayed until after the patient is no longer in the clinic. System-Level Interventions While none of the system-level intervention studies explicitly addressed potential adverse effects of implementing the interventions or reported on the time burden associated with developing, deploying or using them, one study reported a decrease in ordering in rapid 103 streptococcal tests associated with their system-level intervention. There was no difference in the proportion of physicians in the intervention versus control groups ordering chest radiographs however (21. Multifaceted Interventions No study using multiple interventions explicitly measured adverse consequences of the time burden used to create and implement the intervention, although some discussed dropout rates and participation rates, which may be related. Seven studies described the amount of time required by participants to engage in the intervention, undergo training sessions, or participate in site visits or 41,79,102,129,146,147,154,167,168 workshops. Times ranged from 5?10 minutes for patient-focused 41,102 interventions and anywhere from 30 minutes to 1 day for provider-focused interventions 167 146,147 79 including physician education, academic profiling, evidence based training, and 154 training to implement clinical tools. Point-of-Care Tests Combined With Other Strategiesthe studies of multifaceted interventions including a testing component did not specifically measure or report on measures of resource use associated with ordering and interpreting tests. The communication training was accompanied by video demonstrations of consultation techniques and an interactive booklet to use during consultations. Mean number of minutes spent on the training Web site was statistically significantly higher for the combination training group (39. The factors used to determine the overall strength of evidence grades are summarized in Appendix J. Changes in overall prescribing were reported in all studies, while attempts to measure changes in appropriate or inappropriate prescribing were reported in nine studies (7%), and antibiotic resistance was reported in one study. In addition to the sparseness of reporting on the outcome of appropriate prescribing, the few studies that attempted to assess appropriate prescribing had important limitations in outcome definition and ascertainment methods and lack of consistency in methods across studies. Reporting on actual use of antibiotics by the patient was also rare; only studies of delayed prescribing report patient self-report of filling the prescription, with use assumed. Based on the direction and strength of evidence for benefits (prescribing and/or resistance) and adverse consequences (e. For all outcomes, although we sought to determine whether strategies differed based on various patient, clinical, and contextual factors, this was not possible due to the potential confounding influences of a wide variety of other factors. Given the large number of interventions to consider, those with insufficient evidence are not discussed here.
Jatiphala (Nutmeg And Mace). Carbamazepine.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96767