
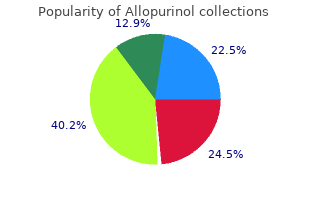
Goldey-Beacom College. V. Avogadro, MD: "Buy online Allopurinol no RX - Safe Allopurinol".
The incidence of thrombocytopenia with eptifibatide and tirofiban is similar to placebo order allopurinol 100 mg online gastritis long term, with rates ranging from 0 purchase allopurinol 100 mg online gastritis diet ���. With abciximab buy allopurinol 100 mg without a prescription gastritis vitamin c, the incidence is reported as 5%; however, up to 4% of cases can be due to pseudothrombocytopenia as a result of platelet clumping. The onset of thrombocytopenia usually occurs within the first 24 hours of infusion, but delayed onset has been reported [34]. Platelet or red blood cell transfusions may be warranted for patients with persistent thrombocytopenia or clinically significant bleeding and must take into account drug concentrations in the plasma or drug bound to platelets [28]. Cilostazol is indicated for treatment of intermittent claudication symptoms and has shown benefit in reducing symptoms and improving walking distance [37]. Dipyridamole is indicated as adjunctive therapy for the prevention of thromboembolism in patients with cardiac valve replacement. Complications and Reversal of Effect Vorapaxar has a long half-life (165 to 311 hours) with 50% inhibition of platelet aggregation recorded for as long as 4 weeks after discontinuation of therapy [21,35]. Nonhemorrhagic complications of cilostazol therapy include headache, peripheral edema, and tachycardia [37]. While headache is the most common adverse effect associated with dipyridamole therapy, hemorrhage may also occur. Anticoagulant agents inhibit thrombosis and propagation by inhibiting thrombin directly or indirectly by attenuating thrombin generation. Each pathway generates a series of reactions in which inactive circulating enzymes and their cofactors are activated. Thrombin plays a pivotal role by triggering the conversion of soluble fibrinogen in insoluble fibrin monomers, which serve as the foundation for thrombus formation. Anticoagulants, either through their interaction with antithrombin, or through a direct inhibition of thrombin, interrupt these enzymatic reactions. Despite these limitations, intravenous administration rapidly achieves therapeutic plasma concentrations that can be monitored and adjusted based on infusion rates [42]. Such nomograms have been associated with a shorter time to reach a therapeutic level without an increase in bleeding events. Patient-specific risk factors for bleeding include age, gender, renal failure, low body weight, and excessive alcohol consumption [47]. Perioperative anticoagulation must be individualized based on the surgery or procedure and the patient’s risks for thrombosis and bleeding. Allergic responses to protamine are more common in patients who have been previously exposed to the drug, but patients can be pre-treated with corticosteroids and antihistamines [41,49]. Anti-Xa monitoring is optional in high-risk patient populations, specifically renal insufficiency, obesity, and pregnancy. In these cases, peak anti-Xa plasma levels are drawn 4 hours after administration, and subsequent doses are adjusted to a target range of 0. Trough levels can be assessed to determine clearance in surgical, procedural, and patient bleeding scenarios. This agent acts as a hemostatically inactive factor Xa decoy that binds free oral direct Xa inhibitors [54]. Patients receiving heparin for a period of greater than 1 month are at risk for developing osteoporosis and vertebral fractures. This results in neutralization of factor Xa, which ultimately inhibits thrombin formation and thrombus development [41]. After subcutaneous administration, fondaparinux has a half-life of 17 to 21 hours in patients with normal renal function. Laboratory monitoring of fondaparinux-specific anti-Xa assays is not recommended on a routine basis, although high-risk patients may warrant monitoring (Table 93. No antidote exists for fondaparinux-related hemorrhage and reversal is further complicated by its prolonged half-life (Table 93. The use of fondaparinux and neuraxial anesthesia or analgesia should follow the conditions used in clinical trials as closely as possible [27]. They selectively bind to the active site of factor Xa and prevent the interaction with prothrombin [40]. Compared to indirect Xa inhibitors such as fondaparinux, these agents do not require antithrombin as a cofactor and inactivate both free and clot-bound factor Xa [40]. These agents have varying degrees of renal and hepatic elimination, elimination half-life, and susceptibility to drug interactions [40,57]. Oral direct Xa inhibitors were developed to provide more stable pharmacokinetic and dynamic profiles that eliminate the need for routine monitoring. Nevertheless, for patients undergoing invasive procedures or for critically ill patients with altered organ function, drug monitoring may be necessary [39]. Calibrated chromogenic anti-Xa assays provide a means to potentially monitor activity; however, exact therapeutic targets have yet to be described in practice [39]. Clinical Indications Available agents include apixaban, edoxaban, and rivaroxaban, which are approved for the prophylaxis and treatment of thromboembolism in a variety of clinical settings (Table 93. These agents have demonstrated a lower rate of intracranial bleeding compared to warfarin; however, the rates of gastrointestinal bleeding were higher compared to warfarin [21,39]. Andexanet alfa is a modified recombinant form of factor Xa currently under investigation for reversal of oral direct acting Xa inhibitors [53,54]. This agent acts as a hemostatically inactive factor Xa decoy that binds free oral direct Xa inhibitors [54]. They exert their antithrombotic effect by binding to the active site of thrombin and inhibiting thrombin-catalyzed reactions. Bivalirudin has the shortest half-life, making it a particularly useful agent in the procedural or periprocedural period. Critically ill patients typically require lower doses than those recommended by the manufacturer [41,59,60]. A humanized monoclonal antibody fragment (Fab) that selectively binds to and inhibits the activity of dabigatran (idarucizumab) only is currently commercially available [53,61]. Removal of dabigatran with hemodialysis or hemoperfusion has been reported to reverse its effects [54]. This laboratory interaction has misled clinicians to discontinue argatroban therapy prematurely, predisposing patients to venous limb gangrene [60]. Since thrombin has a longer half-life (60 to 72 hours) compared to the other factors (6 to 24 hours), at least 6 days of warfarin treatment is required for an antithrombotic effect [62]. In critically ill patients, alterations in coagulation factors, caused by reduced dietary vitamin K intake, hypoalbuminemia, antibiotic administration, acute hepatic injury, or hypermetabolic states, will impact the effects of warfarin. To prevent excessive anticoagulation, loading doses are avoided and low doses are employed for the elderly [44]. Complications and Reversal of Effect Treatment with warfarin increases the risk of major bleeding by 0. Important risk factors for hemorrhage include anticoagulant intensity, time within therapeutic range, and patient age. In patients scheduled for surgery, warfarin may be continued, interrupted for approximately 5 days, or replaced with short-term parenteral or subcutaneous heparinoid bridge therapy depending on the patient’s risk for venous or arterial thromboembolism [14]. Recent findings suggest that the thromboembolism risk during warfarin treatment interruption may be overstated and bridging anticoagulation unnecessary in selected patient populations [68,69].

LeRoith D: Beta-cell dysfunction and insulin resistance in type 2 diabetes: role of metabolic and genetic abnormalities buy allopurinol 100 mg gastritis symptoms fatigue. Diabetes Control and Complications Trial Research Group: the effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus purchase allopurinol 300 mg gastritis diet cookbook. Genuth S order allopurinol 100mg fast delivery gastritis symptoms bupa, Eastman R, Kahn R, et al; American Diabetes Association: Implications of the United Kingdom prospective diabetes study. Lacara T, Domagtoy C, Lickliter D, et al: Comparison of point-of-care and laboratory glucose analysis in critically ill patients. Kurahashi K, Maruta H, Usuda Y, et al: Influence of blood sample oxygen tension on blood glucose concentration measured using an enzyme-electrode method. Kanji S, Buffie J, Hutton B, et al: Reliability of point-of-care testing for glucose measurement in critically ill adults. Langouche L, Vanhorebeek I, Vlasselaers D, et al: Intensive insulin therapy protects the endothelium of critically ill patients. Kanji S, Singh A, Tierney M, et al: Standardization of intravenous insulin therapy improves the efficiency and safety of blood glucose control in critically ill adults. Annane D, Cariou A, Maxime V, et al: Corticosteroid treatment and intensive insulin therapy for septic shock in adults: a randomized controlled trial. Kagansky N, Levy S, Rimon E, et al: Hypoglycemia as a predictor of mortality in hospitalized elderly patients. Tanaka K, Kawano T, Tomino T, et al: Mechanisms of impaired glucose tolerance and insulin secretion during isoflurane anesthesia. Baldwin D, Villanueva G, McNutt R, et al: Eliminating inpatient sliding-scale insulin: a reeducation project with medical house staff. In addition to being life- threatening conditions, they account for thousands of hospitalizations and substantial costs [1]. Recognition of these diabetic comas is particularly important because these conditions are reversible with appropriate treatment. We use diabetic coma as a generic term that encompasses both frank coma and the milder metabolic abnormalities that precede loss of consciousness. This chapter considers the hyperglycemic crises; hypoglycemia and alcoholic ketoacidosis are discussed in Chapter 138. There is frequent overlap of the clinical phenotypes, and clinicians should be aware of this concept [1,2]. For a comatose patient with a blood glucose concentration of less than 50 mg per dL or if for any reason the blood glucose cannot be measured rapidly, the first diagnostic and therapeutic step should be the infusion of 50 mL of a 50% dextrose solution, or when intravenous is not available, injection of 1 mg glucagon intramuscularly or subcutaneously. The hypoglycemic patient who awakens is resuscitated; coma of any other origin is not adversely affected. Deaths are associated with intercurrent heart disease or infection of older patients and cerebral edema of younger patients. Pathophysiology and Etiology Normal Glucose Homeostasis After a meal, pancreatic islet β cells release insulin into the circulation, enabling fuels to enter cells and activating enzymes for their storage or metabolism. Glucose enters most tissues only in the presence of insulin; erythrocytes, heart, and brain are exceptions. In adipose tissue, insulin activates lipoprotein lipase, which clears lipoproteins from the circulation, and stores the triglycerides intracellularly. Insulin has similar effects on skeletal muscle, permitting both amino acids and glucose to enter cells for oxidation or storage [5,6]. During starvation, insulin concentrations decrease, catabolic pathways are activated, and stored fuels (glucose, amino acids, and fats) are mobilized to meet energy needs. Muscle glycogen is not directly available due to lack of glucose-6-phosphatase in muscle cells because glucose-6-phosphate cannot cross the plasma membrane. To support plasma glucose, muscle glycogen undergoes anaerobic glycolysis, generating lactate which can cross the plasma membrane and be converted into glucose in the liver. After glycogen stores are exhausted, the liver synthesizes glucose from muscle-derived amino acids through the process of gluconeogenesis [7]. To conserve muscle mass during starvation, glucose consumption is reduced and fatty acids released from adipose tissue become the principal fuel source. As circulating glucose concentration decreases, insulin concentration also decreases—but never to zero. Low insulin levels permit lipolysis and proteolysis while stimulating gluconeogenesis, all to maintain normal glucose concentrations. Increased glucose concentration stimulates insulin secretion, which in turn reduces or halts catabolism. Precise regulation of insulin secretion, even in the absence of food intake, achieves continuous control of carbohydrate metabolism. When the renal threshold for glucose is exceeded (180 to 200 mg per dL), an osmotic diuresis ensues and water and electrolytes are lost. If insulin deficiency persists, the stress-response hormones cortisol, epinephrine, norepinephrine, glucagon, and growth hormone are released and accelerate catabolism. New-onset type 1 diabetes commonly presents as ketoacidosis, but most cases occur among individuals known to have diabetes. Dietary indiscretion of a person with known treated diabetes may produce classic hyperglycemia, polydipsia, and polyuria but not ketosis. Ketoacidosis occurs most often among patients who have omitted their insulin or who have an intercurrent infection [9]. African Americans with type 2 diabetes may be particularly susceptible to the development of ketosis [11,12]. Other factors that can precipitate ketosis include acute myocardial infarction, emotional stress, cancer, drugs that interfere with insulin release or action, pregnancy, menstruation, and various endocrinopathies. They have typically lost large quantities of fluid; their skin, lips, and tongue are dry; and their eyes are soft to palpation. Abdominal pain is common and may be accompanied by a tender guarded abdomen with diminished or absent bowel sounds. Acute sinusitis and a black intranasal eschar should suggest mucormycosis, an opportunistic fungal infection that disseminates rapidly in acidotic patients. Fingerstick blood glucose determinations are performed on whole capillary blood, and most meters correct for this offset. Because sodium resides principally in the extracellular fluid space, elevated sodium concentration may simply reflect the degree of free water loss. Abnormally low sodium concentrations may be due to the osmotic effect of large amounts of extracellular glucose. The osmotic activity of glucose, drawing free water from the intracellular to the extracellular space, produces a fall of 1. The “corrected” serum sodium of a patient with a measured concentration of 135 mEq per L and a glucose concentration of 600 mg per dL is [1. The patient presenting with an elevated serum sodium concentration despite hyperglycemia has a severe total body free water deficit. Sodium resides only in the aqueous phase of plasma and when the nonaqueous constituents such as triglycerides increase substantially, the reported concentration of sodium will be spuriously low with older testing methods.

The use of cellulitis purchase allopurinol 300 mg without a prescription symptoms of gastritis flare up, length of hospital stay and lymphoedema when these flaps to fill considerable defects and a more con- sentinel node sampling is compared with inguinofemoral servative approach to excision have resulted in less lymphadenectomy purchase cheapest allopurinol and allopurinol gastritis diet journals. As yet it has not Less radical approaches to the vulva have certainly been possible to demonstrate that this translates into improved cosmesis and subsequent function buy generic allopurinol 100 mg gastritis endoscopy. Other improved psychological well‐being, although the surgical modifications [65] to reduce morbidity include psychological trauma of radical excision without sparing the saphenous vein at the time of surgery to reconstruction is well documented [68]. For lymphocyst, a conservative approach is Lymphocyst adopted and drainage under antibiotic cover is recom- Lymphoedema mended only for symptomatic cases, but they tend to Vulval resection re‐form. Wound breakdown/cellulitis Wound healing can be promoted with manuka honey Rectocele dressing [69]. Recently, there have been anecdotal Urinary problems reports of using tissue sealant to promote healing in Psychological groin wounds that have broken down [70]. However, there are data quite clearly indicating certain circumstances, be the sole treatment, but more that squamous vulvar cancers are sensitive to both radio- usually it is used preoperatively with a view to allowing therapy and chemotherapy. Basal cell cancers are well recognized as being radio- Encouraging results were reported by Beriwal et al. All but one remained disease‐free at 26 to respond and verrucous cancers have been reported months. In the remaining 17 patients, who had only a as becoming much more aggressive as a result of partial response, eight developed recurrence locally radiotherapy. Radiotherapy may also be of use in place of surgery for Adjuvant radiotherapy histologically proven involved groin lymph nodes. Whether such irradiated nodes require removal after the factors influencing the need for adjuvant radio- treatment remains unknown. There is insufficient evidence to recommend adjuvant local therapy routinely in patients with subop- Radiotherapy and chemotherapy schedules timal surgical margins (<8 mm). Adjuvant treatment for positive margins is associated with improved survival Radical treatment usually requires that a prophylactic when compared with observation alone [71]. A more dose (45–50Gy) is delivered to the primary and nodal recent multicentre retrospective study of 257 patients sites and the tumour is then boosted by a second phase concluded that in patients with close or positive mar- of treatment using electrons, conformal radiotherapy or gins the addition of adjuvant radiotherapy improved brachytherapy to a total dose of 65Gy. With regard to the use of con- or more lymph nodes are involved with microscopic current chemotherapy and radiation therapy, there are metastatic disease or there is complete replacement and/ no robust prospective data. Treatment have suggested that there may be some improvement in should be to the groins and the pelvic nodes, although local control with regimens employing cisplatin and 5‐ there is no evidence to show whether treatment should fluorouracil, mitomycin C and 5‐fluorouracil, and 5‐ be directed at both sides or to the involved side only. Germany evaluated 1618 patients of whom 1249 had surgical groin staging and known lymph node status. Complications of radiotherapy Node‐positive patients receiving adjuvant radiation (N=189) fared better than 61 patients who did not the reason for the limited application of radiotherapy in receive adjuvant radiotherapy (progression‐free survival this disease lies in the poor record of tolerance and high 39. This difference is significant and the levels of complications reported in the older series. This authors concluded that the addition of chemotherapy almost certainly relates to the type of treatments and would be likely to improve outcome further given the techniques available in these series. More modern equip- incremental improvements seen with other squamous ment and a greater understanding of its potential and cancer [75]. A subsequent study appears to lend weight applications have resulted in a marked improvement in to this assumption where, in a large retrospective cohort tolerance and morbidity [79]. Proctitis is managed with (second field tumour) or as a direct result of tumour prednisolone (Predfoam), Normacol and loperamide. Further work More severe side effects include necrosis of bone (sym- is in progress to develop a clearer understanding of the physis and femoral heads) and fistula formation. Careful bio‐instability of adjacent epithelium and with it the planning of field sizes, dose and fractionation minimize potential for prophylaxis to reduce local recurrence risk. Treatment Recurrent disease the management of relapsed disease will depend on the site and extent of the recurrence [83]. If excision the groin nodes accounting for almost 20% and the would risk sphincter function, radiotherapy should be remainder of relapses occurring in the pelvis or as dis- considered as the first choice. In a large prospective cohort of well‐ been given to maximum dose, then excision should be characterized unifocal cancers in the Groins V2 study, considered. In patients who have not been Most recurrences occur 2 years after primary treat- treated previously with groin irradiation, radiotherapy ment, and close surveillance every 3 months in the first 2 (with or without additional surgery) would be the pre- years is usually practised. The options are much more limited in surveillance for a further 2–3 years and annually thereaf- those who have already been irradiated and palliation, ter. Additionally, patients are encouraged to self‐inspect which may include surgery, should be considered. Survival is poor following regional relapse, hence the efforts to prevent this at the outset. Skin bridge recur- rence has been reported to be more likely to occur in patients with positive lymph nodes [81]. Furthermore, some features of the original dis- margins of at least 8 mm after fixation. In a large ● One lymph node replaced or breached by a tumour or retrospective cohort [54] we have also documented this two with microscopic deposits should prompt adju- phenomenon. Furthermore, the cause functional compromise should have treatment minimum follow‐up was 5 years. It appeared from an individualized (surgery, radiotherapy and chemother- in‐depth analysis that both local recurrence and re‐ apy) to maximize cure and minimize functional occurrence were significantly more likely in women who compromise. Lymph node positivity was also a sig- sion or radiotherapy, whichever would be associated nificant predictor for local relapse. Background Vaginal cancer is rare and accounts for only 1–2% of all Site and size gynaecological malignancies. The upper mous cancers or are the result of extension from the cer- third of the vagina is the site most frequently involved, vix or vulva. Most authors report a wide age range (18–95 either alone or together with the middle third in approxi- years), with the peak incidence in the sixth decade of life mately two‐thirds of cases. As with site, the size of tumour shows great variation Aetiology at presentation, ranging from small ulcers less than a centimetre in diameter to large pelvic masses, although the cause of vaginal cancer is unknown, although sev- the majority of tumours are a maximum of 2–4cm in eral predisposing and associated factors have been noted: diameter. Any tumour classified as a primary vaginal carcinoma should not involve the uterine cervix. There should be no Several authors report that approximately one in four clinical evidence that the tumour represents metastatic or as high as one in three patients have had a previous or recurrent disease. This classification have not been able to confirm pelvic radiotherapy, previ- is summarized in Table 60. The symptoms will depend on the stage of tumour at Differences also exist in interpretations of the signifi- presentation. The most common presenting features are: cance of positive inguinal nodes and their effect on stag- ing.
Syndromes
Importantly cheap allopurinol 100mg without a prescription gastritis diet menu, this study demonstrated peritoneal dissemination within the abdominal cavity order generic allopurinol online gastritis erosive diet. The common factor is that all have intraperitoneal paclitaxel with intravenous bevacizumab Surgical and Medical Management of Epithelial Ovarian Cancer 895 (Arm 3) allopurinol 100 mg overnight delivery gastritis diet using frozen. This followed a number of clinical tri- whether upfront debulking or neoadjuvant chemother- als in heavily pretreated relapsed ovarian cancer patients apy is preferred. Palliation and optimization of quality of life 896 Gynaecological Cancer are important considerations in this clinical scenario, improvement in survival for carboplatin and paclitaxel including careful symptom management and the judi- as front‐line chemotherapy in advanced ovarian cancer. Tumour that has ommended for patients relapsing more than 12 months relapsed more than 12 months following prior treat- from last chemotherapy [106]. Other strategies include Platinum‐sensitive recurrence replacing platinum with an alternative cytotoxic such as Platinum‐sensitive recurrence has several definitions. Although toxicity of the combination biological predictors were the main determinants of sub- was higher than in those receiving olaparib alone, this sequent response, with the treatment‐free interval cor- study gave an indication that the spectrum of activity of relating closely with tumour size. The recently reported benefit was conducted in patients relapsing more than 6 months of niraparib maintenance (see above) in those with a after last chemotherapy. Surgical and Medical Management of Epithelial Ovarian Cancer 897 Platinum‐resistant recurrence longer survival compared with surgery leaving any post- There are various definitions of platinum‐resistant operative residual disease (median 45. These findings recurrent disease requiring treatment within 6 months challenge clinicians to accurately identify those patients of completing last chemotherapy. For this to benefit (or fail to benefit) equally from all convention- reason, based on a multivariate model, three clinical ally dosed and scheduled chemotherapeutic agents. Participating number of novel approaches, including using immuno- centres prospectively enrolled patients with platinum‐ therapy (discussed below). While tion was 76%, thus confirming the validity of this score many supporters of surgical cytoreduction at relapse regarding positive prediction of complete resectability in advocate that complete tumour resection may result more than two‐thirds of patients [117]. The situation is even vaguer in the tertiary bosis rate, while 52% of the patients required postopera- setting and beyond. There are future plans to combine results significance for complete tumour resection, whilst from both trials to achieve a larger cohort and more residual tumour at secondary and tertiary surgery, robust survival data. Despite these encouraging retrospective data it is still not clear if Management of bowel obstruction the surgery itself is influencing survival or whether oper- in the palliative setting ability is just a surrogate marker of more ‘favourable’ tumour biology and therefore a better overall prognosis. The most frequent tumour dissemi- proximal ileostomy or jejunostomy since, due to peri- nation site was the pelvis (73%). Most importantly, common institutional and physical resources and consideration of clinicopathological characteristics such as tumour stage, total parenteral nutrition. Benefits should be very carefully stitute a selection bias since patients who are fit enough balanced with risks for each individual patient. Factors to tolerate chemotherapy following radical surgery may such as comorbidities, baseline quality of life, previ- have more favourable survival rates than those for whom ous response to chemotherapy, treatment intervals and chemotherapy was contraindicated. The most common complications were infection/ bowel obstruction, a single stent or stoma formation is sepsis (13%) and re‐laparotomy (4. Here, further options such as percutane- without any higher rates of thromboembolic events ous endoscopic gastrostomy can used in highly selected (2. Despite this, improvements have been noma, renal cell cancer and non‐small cell lung cancer. In a study by Hamanishi the most lethal of gynaecological cancers, warrant- et al. Only then can therapies be rationally in combination with chemotherapy, targeted therapies designed or improved to make a significant impact on and other immune activators are currently underway the outcome of this most deadly of cancers. Ovarian cancer is a 6 Beral V, Million Women Study Collaborators, Bull D, heterogeneous disease. Global cancer Cancer incidence and mortality in relation to body mass statistics, 2002. Facts Views Vis Obgyn 8 Collaborative Group on Epidemiological Studies of 2013;5:292–297. Menopausal hormone use and ovarian 5 Collaborative Group on Epidemiological Studies of cancer risk: individual participant meta‐analysis of 52 Ovarian Cancer. Acta Obstet Gynecol Scand versus delayed treatment of relapsed ovarian cancer 2006;85:93–105. Precursors and pathogenesis of ovarian carcinogenesis: revisited, revised, and expanded. Novel molecular ovarian mucinous and transitional cell (Brenner) subtypes of serous and endometrioid ovarian cancer neoplasms and their relationship with Walthard cell linked to clinical outcome. Am J carcinoma of the fimbria and pelvic serous carcinoma: Gastroenterol 2001;96:253–254. Precursors of ovarian cancer in the fallopian tube: Surgical and Medical Management of Epithelial Ovarian Cancer 901 serous tubal intraepithelial carcinoma. Rethinking candidate precursor to pelvic serous cancer (p53 ovarian cancer: recommendations for improving signature) and its prevalence in ovaries and fallopian outcomes. Best Pract Res Clin Obstet Gynaecol predicting suboptimal cytoreductive surgery in women 2006;20:321–338. Prophylactic bilateral reciprocal validation study of computed tomography salpingectomy as a prevention strategy in women at predictors of suboptimal primary cytoreduction in high‐risk of ovarian cancer: a mini‐review. Surgical outcome Staging classification for cancer of the ovary, fallopian prediction in patients with advanced ovarian cancer tube, and peritoneum. Int J Gynaecol Obstet using computed tomography scans and intraoperative 2014;124:1–5. Q J Nucl Med Mol Imaging Managing Breast Cancer and Related Risks in People 2016;60:93–102. Int J Gynecol Cancer Adjuvant (post‐surgery) chemotherapy for early stage 2010;20:1142–1147. J Natl study of systematic lymphadenectomy in patients with Cancer Inst 2005;97:560–566. Lymph node metastasis in stages I and surgical cytoreduction for advanced ovarian carcinoma. Lymph node metastasis in stage I epithelial chemotherapy versus primary surgery for newly ovarian cancer. The a combined exploratory analysis of 3 prospectively optimal organization of gynecologic oncology services: randomized phase 3 multicenter trials: by the a systematic review. The effect intergroup trial of cisplatin–paclitaxel versus cisplatin– of debulking surgery after induction chemotherapy on cyclophosphamide in women with advanced epithelial the prognosis in advanced epithelial ovarian cancer. Paclitaxel plus carboplatin versus standard surgery for advanced ovarian carcinoma during the chemotherapy with either single‐agent carboplatin or Surgical and Medical Management of Epithelial Ovarian Cancer 903 cyclophosphamide, doxorubicin, and cisplatin in 100 Ledermann J, Harter P, Gourley C et al. Lancet maintenance therapy in platinum‐sensitive, recurrent Oncol 2015;16:928–936. Clinical paclitaxel once a week in combination with carboplatin trials in recurrent ovarian cancer. Int J Gynecol Cancer every 3 weeks for advanced ovarian cancer: a phase 3, 2011;21:771–775. Intraperitoneal cisplatin and paclitaxel in ovarian Paclitaxel plus platinum‐based chemotherapy versus cancer. Gynecol secondary cytoreductive surgery in recurrent ovarian Oncol 2009;112:265–274.
Order allopurinol 100 mg without a prescription. Endoscopy of a Gastric Cancer.