
Michigan State University. U. Ines, MD: "Purchase cheap Ezetimibe no RX - Cheap Ezetimibe no RX".
Insomnia Page 10 of 86 Final Report Update 2 Drug Effectiveness Review Project Figure 1 discount ezetimibe 10mg with amex cholesterol test cost in india. Newer drugs for insomnia: Results of literature search 2570 citations identified through searches 2 cheap ezetimibe cholesterol levels checked at home,200 excluded at title/abstract level 370 retrieved for full-text evaluation 165 excluded at full-text level: 44 no original data (letter generic ezetimibe 10 mg mastercard cholesterol panel ratio, editorial, nonsystematic review, etc. One trial is published as a poster 18 presentation only; additional details were provided by the manufacturer and in the FDA review 20 of eszopiclone. Total numbers of head-to-head trials of newer drugs for insomnia Zolpidem extended Zaleplon Zolpidem release Zopiclone Eszopiclone Ramelteon Zaleplon ********* Zolpidem 4 ********** Zolpidem extended 0 0 ********** release Zopiclone 0 3 0 ********** Eszopiclone 0 1 0 0 ********** Ramelteon 0 0 0 0 0 ********** We included 44 trials in 45 publications comparing newer insomnia drugs compared with 21-65 benzodiazepines. Appendix D summarizes the efficacy, safety, and rebound insomnia results of these studies. We identified two trials comparing trazodone compared with a sedative hypnotic; one 52 61 (compared with zaleplon) was rated poor quality and the other (compared with zolpidem) was rated fair. The review most relevant to this report is a comparative review conducted by the National 124 Institute for Clinical Excellence. The others were not designed to compare the sedative hypnotics head-to-head. One meta-analysis examined the risks and benefits of sleep agents, 126 including newer sedative hypnotics, in older people with insomnia. We included 20 observational studies of adverse events associated with newer drugs for 127-146 insomnia. Insomnia Page 12 of 86 Final Report Update 2 Drug Effectiveness Review Project Key Question 1. What is the comparative effectiveness of newer drugs in treating adults and children with insomnia? Summary of the Evidence There is no evidence in children. Direct evidence • Direct evidence is from 8 short-term head-to-head trials (7 fair quality, 1 poor; 1 measured withdrawal effects only) • Eszopiclone compared with zolpidem (1 trial) - There was no significant difference between eszopiclone 2 mg or 3 mg and zolpidem 10 mg on polysomnography-measured sleep latency, WASO, or number of awakenings. We were unable to include data from these trials in the adjusted indirect analysis. A post hoc analysis found that WASO was significantly better than placebo through hour 6, although not at hours 7 and 8 • Results for subjective sleep outcomes were mixed, with zolpidem extended-release showing superiority to placebo at some, but not all, assessment points • In patients over age 65, polysomnography-measured WASO was shorter than placebo through the first 6 hours of the night • In a 6-month study of intermittent treatment (3 to 7 nights per week), 90% of patients taking zolpidem extended-release said the treatment helped them sleep, compared with 51% of the placebo group Detailed Assessment Direct evidence Patient and study design characteristics of included head-to-head trials are shown in Table 3. No new head-to-head trials were identified for Update #2. Insomnia Page 14 of 86 Final Report Update 2 Drug Effectiveness Review Project Table 3. Head-to-head trials of newer insomnia drugs: Study design and patient characteristics Study, year Treatment (Quality) Study arms Design Population duration Primary outcome Eszopiclone 1 mg Erman Eszopiclone 2 mg N=65 (poster and polysomnography- Eszopiclone 2. According to the study funder, the objective of the study was to evaluate the polysomnographic efficacy and safety of eszopiclone relative to placebo. Zolpidem 10 mg was included as an active control to allow qualitative comparisons to eszopiclone. The primary efficacy outcome was latency to persistent sleep as measured by polysomnography. The study compared 4 doses of eszopiclone (1 mg, 2 mg, 2. Insomnia Page 15 of 86 Final Report Update 2 Drug Effectiveness Review Project Both drugs were more effective than placebo for the primary outcome of polysomnography-measured sleep latency. There was also no difference between zolpidem and eszopiclone on subjective measures of next-day effects, including morning 20 sleepiness, daytime alertness, and daytime ability to function. The main analysis in this study compared eszopiclone with placebo; no analysis comparing eszopiclone with zolpidem was presented. To make a direct comparison between the two drugs, we calculated the weighted mean difference between eszopiclone and zolpidem for polysomnography-measured sleep outcomes using data provided in the FDA review of 20 eszopiclone. There were no significant differences between eszopiclone and zolpidem on polysomnography-measured sleep latency, WASO, or number of awakenings. Subjective measures were also reported, but standard deviations were not provided, so we could not calculate a mean difference. Head-to-head comparison of eszopiclone compared with zolpidem on 147 polysomnography-measured outcomes Mean (SD) at endpoint (P value compared with placebo) Eszopiclone 2 mg Eszopiclone 3 mg 1. Zolpidem 10 mg mean difference mean difference Outcome 4. Zaleplon compared with zolpidem 12, 14, 15, 17 Four fair-quality head-to-head studies compared zolpidem with zaleplon and placebo. The fourth head-to-head study was a small, single-dose crossover trial that measured patient preference as a primary outcome. In the 3 studies with sleep outcomes, comparisons between zaleplon and placebo were the primary comparisons. Published reports do not provide a head-to-head analysis comparing Insomnia Page 16 of 86 Final Report Update 2 Drug Effectiveness Review Project zaleplon with zolpidem, and it was not possible to conduct an analysis of zaleplon compared with zolpidem from data provided. Sleep latency was the primary outcome in two studies in adults. Both compared zaleplon at three fixed doses (5 mg, 10 mg, or 20 mg) with zolpidem 10 mg for 4 weeks. A placebo arm was also included, and analyses are presented for the comparison to placebo. Neither publication provided a head-to-head analysis of zolpidem compared with 5 zaleplon, but a head-to-head analysis is provided in the FDA statistical review of zaleplon for 15 15 one trial. At weeks 1 through 4, there was no difference between zaleplon 5 mg or 10 mg and zolpidem 10 mg on the median number of minutes to sleep onset. The only significant difference between the drugs on this outcome was a shorter latency with zaleplon 20 mg compared with zolpidem 10 mg. There was no difference in the comparison of recommended starting doses zaleplon 10 mg and zolpidem 10 mg. These results are not from intention-to-treat analyses. Zaleplon at all three doses had a shorter latency than placebo at all time points, with the exception of 5 mg at week 4. For zolpidem 10 mg, at weeks 2 and 3 latency was significantly shorter than for placebo but was not significantly different at week 4. At week 1, there was a trend for shorter latency, but this was not significant (-10 minutes; P=0. In a 2-week head-to-head trial of zaleplon 5 mg or 10 mg compared with zolpidem 5 mg 12 conducted in 549 older adults (65 years or older), results were similar to those of the trials in younger patients. There was no difference in sleep latency for zaleplon 5 mg and zolpidem 5 mg, but zaleplon at a higher dose (10 mg) was associated with a shorter latency than zolpidem 5 mg. Zolpidem, but not zaleplon, was associated with rebound sleep latency on the first night of discontinuation. Duration of sleep was a secondary outcome in three head-to-head trials of 12, 14, 15 zaleplon compared with zolpidem.
It may be that an individual patient’s risk of bleeding which inhibits the conversion of vitamin K2 buy genuine ezetimibe online serum cholesterol levels definition,3 epoxide to vitamin K is unrelated to the initial indication for anticoagulation; for example generic 10 mg ezetimibe mastercard good cholesterol ratio but high ldl, quinone buy cheap ezetimibe 10 mg line cholesterol levels versus age, as well as the conversion of vitamin K quinone to vitamin a large observational registry of rivaroxaban use found the major K quinol, the active form of vitamin K. In addition, because the major indications for ing warfarin therapy, the risk of major bleeding in patients long-term TSOAC use are AF and VTE, this review focuses first on anticoagulated with warfarin ranges from 0. Table 1 summarizes the rates of major bleeding, GI devastating form of major bleeding, intracranial hemorrhage (ICH), bleeding, and ICH associated with each agent. This highlights one of the challenges of warfarin therapy in real-world practice. That said, even stable INR is not fully protective and the majority of warfarin-related ICH patients present while in the appropriate therapeutic range,12 so even Direct thrombin (factor IIa) inhibitors successful maintenance in the therapeutic range does not prevent The DTIs are a class of drugs available for both oral and intravenous this devastating complication. Overall, the rate highlighted the importance of ICH as a complication of warfarin; of major bleeding with dabigatran 150 mg bid in the RE-LY trial when major bleeding occurred outside the brain, only 3% was 3. Major bleeding in TSOACs when compared with warfarin: selected studies Risk of major Risk of GI Risk of intracranial Agent bleeding (95% CI) bleeding (95% CI) bleeding (95% CI) All AF32 RR 0. They found that the incidence rate of ICH on and using the TIMI definition, major bleeding occurred in 0. There was Most importantly for the clinician, it is clear that the HR for a signal suggesting an increased incidence of major GI bleeding of bleeding (compared with warfarin) is similar irrespective of defini- 34. Consis- Edoxaban tent with this, it appears that when major bleeding develops, those At the time of this writing, edoxaban is not yet available in the randomized to dabigatran have shorter intensive care unit stays and United States. The ENGAGE AF-TIMI 48 trial21 noted that the rate a trend toward improved mortality compared with patients on of major bleeding was 3. This highlights These drugs inhibit factor Xa, the first step in the common pathway the fact that, as with the other factor Xa inhibitors, the risk of of the coagulation cascade, in a dose-dependent fashion. The risk is slightly lower with factor Xa Overall, the risk of major bleeding associated with VTE therapy inhibitors than warfarin (OR 0. Impor- appears lower with TSOACs than with warfarin [relative risk tantly, the risk of the most severe type of bleeding, ICH, was 22 (RR) 0. Specific factors that modify this substantially lower with TSOACs (OR 0. Therefore, should be applied to those who are older, those with renal although this class of agents is associated with important major insufficiency, and those on concomitant antiplatelet agents or bleeding risks, these risks appear to be consistently lower than those NSAIDs. It is not yet clear whether there are clinically relevant differences in bleeding risks between different factor Xa inhibitors. Direct thrombin (factor IIa) inhibitors For patients on dabigatran for VTE, major bleeding appears to occur Rivaroxaban in 0. Rivaroxaban Apixaban For patients on rivaroxaban for VTE, major bleeding occurred in The ARISTOTLE trial highlighted how major bleeding risk can 0. Indirect comparisons Renal insufficiency Although numerous individual studies compare the bleeding rates Patients with renal insufficiency appear to be at increased major bleeding risk with anticoagulants. For example, the ROCKET-AF population showed higher CHADS2 scores than other trials, suggest- Those with moderate renal insufficiency are at even higher risk, ing a higher-risk population, so that the event rates for rivaroxaban with rates of major bleeding of 6. However, the apparent benefit of TSOACs was less obvious (OR for major bleeding 0. It is Some groups have attempted to compare different agents indi- likely that this finding is due to smaller numbers of patients with rectly using a common comparator (warfarin). However, the point estimate is similar risk to be lower with dabigatran than with rivaroxaban, but this and the trend toward lower bleeding rates with TSOACs is relatively was only significant for the lower 110 mg dose (OR 0. They also noted Some patients are at such increased thromboembolic risk that the risk of major bleeding to be lower with apixaban than with consideration is given to providing both an oral anticoagulant and high-dose dabigatran (OR 0. This issue appears to be most common after an rivaroxaban (OR 0. However, such an approach found similar results, with apixaban being associated with a should be considered with caution because concomitant therapy lower risk of major bleeding than dabigatran (RR 0. This trial was halted early because any benefit was gested that apixaban demonstrates a lower overall bleeding risk outweighed by major bleeding, which increased from 0. For the most part, unlike warfarin, no clinically available tools exist to detect drug levels of the TSOACs. However, it is likely that Advanced age plasma concentration influences bleeding risk. A substudy of the Older patients appear to be at consistently higher risk of bleeding RE-LY study of dabigatran for AF found that the risk of major complications while being anticoagulated. That said, such patients There has been concern that this information was not made available are also at higher risk for thromboembolism and can often derive in a timely manner to the public. Overall, serum concentrations of TSOACs, like high INR levels in warfarin it appears that TSOACs are associated with lower bleeding risks patients, carry elevated bleeding risks, it has been consistently than warfarin for younger patients (RR 0. Incidence of bleeding in trials of AF Study Population Major bleeding Dabigatran Ezekowitz et al45 VKA-naive and experienced individuals with AF VKA-naive: Dabigatran 110 mg: 3. Furthermore, at this time, serum drug levels are not routinely Some modifiable factors include high levels of alcohol intake, drug available to clinicians nor are therapeutic drug target ranges use, and cigarette smoking. Incidence of bleeding in trials of VTE Study Population Major bleeding Dabigatran Schulman et al24 Confirmed VTE Dabigatran: 1. Therefore, all patients on antico- from clopidogrel plus aspirin and from warfarin. Risk of stroke and intracranial hemorrhage in 9727 Chinese with atrial fibrillation in Hong Kong. Dabigatran versus warfarin in In recent years, several novel oral anticoagulants have been patients with atrial fibrillation. A direct comparison of bleeding rates is difficult due to 8. Rivaroxaban versus warfarin in different bleeding definitions and the fact that each major trial used nonvalvular atrial fibrillation. Twelve-month outcomes and appears that the TSOACs have slightly lower rates of overall major predictors of very stable INR control in prevalent warfarin users. J bleeding and ICH in particular, but may carry slightly higher rates of Thromb Haemost. Clinicians seeking to minimize the risk of major 10. Location and outcome of bleeding should consider avoiding concomitant antiplatelet therapy, anticoagulant-associated intracerebral hemorrhage. Warfarin, hematoma expan- sion, and outcome of intracerebral hemorrhage. The effect of warfarin and Conflict-of-interest disclosures: M. Death and disability from warfarin- associated intracranial and extracranial hemorrhages. Goldstein, MD, PhD, Department of Emergency Medi- and outcome of rivaroxaban bleeding in daily care: results from the cine, Massachusetts General Hospital, Zero Emerson Place, Suite Dresden NOAC registry.
Placebo controlled trials of beta blockers for migraine Author Year Age Other population Number screened/ Country Method of outcome assessment Gender characteristics eligible/ Study Design and timing of assessment Ethnicity (diagnosis discount 10 mg ezetimibe mastercard cholesterol in cooked eggs, etc) enrolled Kangasniemi Diary card measuring following n=74 Family history: 54(73%) NR/NR/77 randomized 1987 variables: Mean Attacks per month(mean): 4 purchase ezetimibe with a mastercard cholesterol in medium eggs. Placebo controlled trials of beta blockers for migraine Author Number Year withdrawn/ Method of Country lost to fu/ adverse effects Study Design analyzed Outcomes assessment? Kangasniemi 3 withdrawn(1 due to Outcomes per 4 weeks (mean score/% change) Recorded at each 1987 narcotic abuse and 2 due to Attack frequency: met=1 buy ezetimibe 10mg otc cholesterol in eggs wiki. Placebo controlled trials of beta blockers for migraine Author Withdrawals due Year to adverse events Country (%, adverse Study Design Adverse effects reported n/enrolled n) Comments Kangasniemi Adverse effects NR Classic migraine 1987 incidence(% patients): only Scandinavia met=36%; pla=18% Fair quality Most frequent adverse RCT effects(# complaints for weeks 1-4/5-8) Gastrointestinal: met=7/9; pla=1/2 Fatigue: met=6/7; pla=3/1 Cardiovascular: met=1/2; pla=0/3 Sleep disturbances: met=3/1; pla=0/0 Others: met=10/6; pla=7/8 Beta blockers Page 360 of 494 Final Report Update 4 Drug Effectiveness Review Project Evidence Table 16. Placebo controlled trials of beta blockers for migraine Author Year Allowed other Country Interventions (drug, medications/ Study Design Eligibility criteria Exclusion criteria regimen, duration) interventions Pindolol Ekbom Aged 19-56, with classic or common Bronchial asthma, severe infectious Group 1: Pindolol (pin1) 7. Placebo controlled trials of beta blockers for migraine Author Year Age Other population Number screened/ Country Method of outcome assessment Gender characteristics eligible/ Study Design and timing of assessment Ethnicity (diagnosis, etc) enrolled Pindolol Ekbom Patient record: 1) frequency, 2) Mean Classic migraine=4(13. Placebo controlled trials of beta blockers for migraine Author Number Year withdrawn/ Method of Country lost to fu/ adverse effects Study Design analyzed Outcomes assessment? Placebo controlled trials of beta blockers for migraine Author Withdrawals due Year to adverse events Country (%, adverse Study Design Adverse effects reported n/enrolled n) Comments Pindolol Ekbom NR Withdrawals: pin=4; 1971 pla=0 Sweden Withdrawals due to: Fair quality Orthostatic RCT hypotension=2 Increased headache=1 Dizziness/cystopyel itis=1 Sjaastad Untoward effects noted: pin=3/28(10. Placebo controlled trials of beta blockers for migraine Author Year Allowed other Country Interventions (drug, medications/ Study Design Eligibility criteria Exclusion criteria regimen, duration) interventions Propranolol Borgesen Diagnosis of migraine (Ad Hoc Committee Cardiac disease; asthma or diabetes Propranolol (pro) 120 mg Symptomatic treatments 1974 on Classification of Headache, 1962); mellitus; physical or neurological daily allowed (e. Placebo controlled trials of beta blockers for migraine Author Year Age Other population Number screened/ Country Method of outcome assessment Gender characteristics eligible/ Study Design and timing of assessment Ethnicity (diagnosis, etc) enrolled Propranolol Borgesen Patient forms: 1) severity on 3-point Mean Classical migraine (# pts/%): NR/NR/45 entered 1974 scale (severe=forcing patient to stay age=37. Placebo controlled trials of beta blockers for migraine Author Number Year withdrawn/ Method of Country lost to fu/ adverse effects Study Design analyzed Outcomes assessment? Placebo controlled trials of beta blockers for migraine Author Withdrawals due Year to adverse events Country (%, adverse Study Design Adverse effects reported n/enrolled n) Comments Propranolol Borgesen Data NR; pro=pla for pro=0 1974 #/severity of complaints of pla=2 Denmark fatigue drowsiness and diarrhea Fair quality RCT Crossover Dahlof NR NR Looked at 1987 longlasting Sweden prophylactic effect following Fair quality discontinuance RCT Crossover Beta blockers Page 368 of 494 Final Report Update 4 Drug Effectiveness Review Project Evidence Table 16. Placebo controlled trials of beta blockers for migraine Author Number Year withdrawn/ Method of Country lost to fu/ adverse effects Study Design analyzed Outcomes assessment? Placebo controlled trials of beta blockers for migraine Author Withdrawals due Year to adverse events Country (%, adverse Study Design Adverse effects reported n/enrolled n) Comments Diamond Frequency of most Phases I & II 1982 common adverse events(# combined: United States patients/%) pla=3/245(1. Placebo controlled trials of beta blockers for migraine Author Year Age Other population Number screened/ Country Method of outcome assessment Gender characteristics eligible/ Study Design and timing of assessment Ethnicity (diagnosis, etc) enrolled Diener Headache diary Mean age: pro n=78; pla n=55 235/214/214 1996 pro=40; Mean migraine history(years): Germany pla=39 pro=21; pla=19 % female: Migraine with aura(#/% Fair quality pro=76. Placebo controlled trials of beta blockers for migraine Author Number Year withdrawn/ Method of Country lost to fu/ adverse effects Study Design analyzed Outcomes assessment? Diener 40 withdrawn/0 lost to fu/214 pro n=78; pla n=55 NR 1996 analyzed per ITT; 174 Migraine frequency(#/% patients with >/= 50% reduction of attacks): Germany analyzed per protocol pro=33/42. Placebo controlled trials of beta blockers for migraine Author Withdrawals due Year to adverse events Country (%, adverse Study Design Adverse effects reported n/enrolled n) Comments Diener Overall adverse Overall withdrawals 1996 effects(#/% patients): due to adverse Germany pro=19/24. Placebo controlled trials of beta blockers for migraine Author Year Allowed other Country Interventions (drug, medications/ Study Design Eligibility criteria Exclusion criteria regimen, duration) interventions Forssman Diagnosis of migraine; age between 16 and Pregnancy or suspicion of pregnancy; Propranolol (pro) 240 mg Previously prescribed 1976 55 years; at least three attacks per month indication of renal or heart disease, daily acute medication allowed Sweden hypertension, diabetes or asthma; Placebo (pla) x 12 weeks, (not specified); oral history of earlier treatment of migraine then crossover contraceptives Fair quality with propranolol RCT Crossover Kuritzky Patients aged 17-53, suffering from NR Long acting propranolol (LA Analgesics 1987 classical or common migraine for at least 2 pro) 160 mg daily Israel years with at least 3 attacks per month Placebo (pla) Fair quality RCT Crossover Beta blockers Page 377 of 494 Final Report Update 4 Drug Effectiveness Review Project Evidence Table 16. Placebo controlled trials of beta blockers for migraine Author Year Age Other population Number screened/ Country Method of outcome assessment Gender characteristics eligible/ Study Design and timing of assessment Ethnicity (diagnosis, etc) enrolled Forssman Printed record card: 1) begin/end Mean Classic migraine=5/32(15. Placebo controlled trials of beta blockers for migraine Author Number Year withdrawn/ Method of Country lost to fu/ adverse effects Study Design analyzed Outcomes assessment? Forssman 8(20%) withdrawn/0 lost to Attack frequency of propranolol relative to placebo (# patients/%): Good NR 1976 fu/32 analyzed effect(>/= 50% improvement)=11/34. Placebo controlled trials of beta blockers for migraine Author Withdrawals due Year to adverse events Country (%, adverse Study Design Adverse effects reported n/enrolled n) Comments Forssman Most common side effects pro=2 1976 reported(# pts/%) pla=2 Sweden Increase in weight > 2 kg: pro=5(13. Placebo controlled trials of beta blockers for migraine Author Year Allowed other Country Interventions (drug, medications/ Study Design Eligibility criteria Exclusion criteria regimen, duration) interventions Malvea Age range of 25-57 with common migraine Pregnancy, bronchial asthma, Propranolol (pro)
You should always discuss defibulation with the patient buy ezetimibe with mastercard how much cholesterol in eggs benedict. HIV transmission and female genital mutilation The practice of FGM involves the use of one in- strument for multiple operations under non-sterile conditions and thus carries a high risk of trans- mission of infection including HIV for the women or girls undergoing FGM but as well for the circumcisor purchase generic ezetimibe cholesterol medication zocor. Recently order ezetimibe online pills cholesterol levels us vs canada, there has been a growing interest in the relationship between the practice of female circumcision and the spread of AIDS. POSSIBLE SURGICAL INTERVENTION TO REVERSE FEMALE GENITAL MUTILATION Defibulation Figure 11 Injection of local anesthetic in the scar. Abdul Cader This is a surgical procedure to reverse infibulation by opening the vaginal introitus, uncovering the 3. Identify the midline of infibulation by lifting it urinary meatus and rebuilding, as much as possible, up using a dissecting forceps introduced in the a ‘normal’ anatomy of the external genitals. This vaginal opening and let it slide further under the procedure is especially necessary in patients with scar bridge of the infibulation (Figure 12). The operation is cases where the vaginal opening is not too nar- described step by step below: row you can use your index finger. Careful preoperative disinfection of the peri- to protect the underlying structure (urethra) neal and genital zone with iodate solution. Cut beginning from the bottom upwards several points of the scar (see Figure 11 ). Stop almost 1–2cm above the 280 Female Genital Mutilation urethral orifice. Widen the edge of defibulation daily using symmetry of the incision. Suture the single edge of the incision with welding of incision. Counsel the patient to urinate into a bowl (Monocryl 00) as shown in Figure 13. Restoration of the clitoris The French urologist Dr Pièrre Foldes is the only surgeon who has developed a surgical technique to restore the clitoris5. Place the patient under general anesthesia in lithotomy position. Open the scar on top of the clitoris stump stay- ing closely to the stump, proceeding upwards to include the residual shaft of the clitoris (Figure 14). Remove the scar tissue surrounding the shaft of the clitoris and the suspensory ligament (Figure 15). Mobilize the suspensory ligament by transect- ing it vertically (Figure 16). Fix the neo-clitoral shaft using single stitches with Monocryl on the lateral and inferior border of the shaft (Figure 17). Adapt the skin with interrupted stitches using Monocryl (Figure 17). Figure 12 Incising the infibulated vulva in the midline. Tissue is then removed from the thighs to Source: A. The surgery takes less than an hour in experienced hands and can be done as an outpatient procedure with 1 day in hospital postoperatively. Post-surgery pain may last 2 weeks and 4–6 weeks later, women claim to have a new healthy sexuality and to feel again their clitoris (Figure 18). A study found a positive change in sexual arousal in 75% of the 453 patients6. It is difficult to compare pre- and postoperative results as most patients never experienced a nor- mally functioning clitoris before their operation but patients’ satisfaction with the method could be assessed by using psychometric questionnaires. PREVENTION There are four groups of people who need to be Figure 13 Closing the defibulation. Abdul informed about the consequences of FGM in order Cader to prevent its continuation7: 281 GYNECOLOGY FOR LESS-RESOURCED LOCATIONS (a) (b) Figure 15 Mobilizing the shaft of the clitoris. Ground actors are a cornerstone in the abolition of FGM. By changing their practice and sensitizing the community they can help to stop FGM. Patients often don’t know that their symptoms are related to FGM as they have no way of comparing themselves to a non- circumcised woman in areas of high incidence. They and their families need to learn about that link and about the steps to take, e. Foldes present early in pregnancy to discuss and perform defibulation. Young girls should receive training at school to relate their symptoms to FGM if they had • Health personnel. Communities need to • ‘Ground actors’ [circumcisors, non- governmental be aware of the consequences of FGM as well as organizations (NGOs) like women’s groups, they often do not know this, especially husbands traditional healers, traditional birth attendants]. Healthcare workers, particularly midwives and Health personnel should receive training on the obstetricians, have a dual responsibility: complications of FGM and how to take care of patients presenting to them. They should learn • To help the patients with FGM at the hospitals. Foldes Figure 16 (a, b) Further mobilizing the clitoral shaft. Foldes • To help the families become aware of the services available in the communities. Foldes 283 GYNECOLOGY FOR LESS-RESOURCED LOCATIONS • In some situations, education and informa- 9. African genital mutilation: the unspeakable tion may be helpful in making interventions atrocities. Br J Obstet Gynaecol 1994;101:94–5 words because it is inexpressibly horrible. Foundation for Women’s Health, Research and Develop- ment (FORWARD). Report REFERENCES on the First National Conference on Female Genital Mutilation, 1. Prevalence of female genital mutilation (FGM) in Africa. Eliminating female genital mutilation: an interagency org/? Female genital cutting /mutilation (FGC/ Women’s Health Research and Development, 1992 Royal FGM) continues despite damaging health repercussions. The Tackling female genital mutilation from a health and Unspoken Issue. Cutting the Rose: The Practice and its Pre- damaging-health-repercussions/587/ug.
A uth ors N otreported N umberofexcluded studies not 66 comparative controlled studies employed by reported 1994 th erapeuticprofile of N otclearwh at comparingtiz anidine Sandoz and tiz anidine and oth er meth ods used to with anoth ermuscle A th ena discount ezetimibe american express cholesterol medication injection. Included system aticreviews and m eta-analyses ofskeletalm uscle relaxants inpatients with spasticity A uth or Population Y ear ch aracteristics M ainresults A dverse events Internalvalidity C om m ents Taricco C rossoverstudies: Tiz anidine vs purchase ezetimibe 10 mg cholesterol purpose. M eth ods of 66 45-57% cerebrovascular analysis) controls database search not 1994 disease generic ezetimibe 10 mg cholesterol upper limit,0-7% amyotroph ic M uscle tone (improved): 64% vs. N o quality lateralsclerosis M uscle spasms (improved): 50% vs. N o assessment G ender,age,race not M uscle strength (improved): 34% vs. N ot notreported) clearifstudies O verallassessmentofantispasticeffect summariz ed appropriately: (moderate,good,orexcellent): 67. Included system aticreviews and m eta-analyses ofskeletalm uscle relaxants inpatients with spasticity Tim e period covered F unding A uth or and sources used in Exclusion source and M eth od of C h aracteristics ofidentified Y ear A im s literature search Eligibility criteria criteria role appraisal articles M eta-analyses (notsystem aticreview) G roves A ssess th e efficacy Time period covered C ontrolled,doubled- Studies with out A uth ors N otreported 10 studies excluded. N ot data,th ree key incomplete reported if outcome measures scale formuscle funderh eld (A sh worth R ating strength or data. Scale,measure of tone,no exam muscle strength ,and atsixweeks, G lobalTolerability to and one study TreatmentR ating), inpatients with and patients h ad amyotroph ic multiple sclerosis or lateralsclerosis. Included system aticreviews and m eta-analyses ofskeletalm uscle relaxants inpatients with spasticity A uth or Population Y ear ch aracteristics M ainresults A dverse events Internalvalidity C om m ents M eta-analyses G roves 147 patients with multiple Tiz anidine vs. N o evaluationfor Included studies 69 sclerosis M eanch ange intotalA sh worth score (scale 0 to h eterogeneity. Included system aticreviews and m eta-analyses ofskeletalm uscle relaxants inpatients with m usculoskeletal conditions Tim e period covered and F unding A uth or sources used inliterature source and M eth od of C h aracteristics of Y ear A im s search Eligibility criteria Exclusioncriteria role appraisal identified articles System aticreviews Sch nitz er A ssess th e efficacy Th rough O ctober2002 R C Ts oflow back N otspecified M erck & A bstracted 50 of110 identified R C Ts 60 and safety oflow paininadults th at C ompany, informationon metinclusioncriteria;6 2004 back pain M ultiple databases including used quantitative N ew Jersey; study evaluated skeletal medications M edline,EM BA SE, clinicalendpoints of role offunder ch aracteristics, muscle relaxants C och rane efficacy and/orsafety notreported quality usingK oes criteria (0-100) 6 placebo-controlled trials (1 baclofen,3 tiz anidine,1 ch lormez anone,1 tetraz epam) 931 patients included in6 trials Tofferi A ssess th e efficacy Th rough N ovember2000 Placebo-controlled N otspecified N otreported A bstracted 5 of27 identified R C Ts 62 and safety of R C Ts with informationon metinclusioncriteria 2004 cyclobenz aprine for M ultiple databases including measurable study fibromyalgia M EDL IN E,EM BA SE,DA R E, outcomes ch aracteristics, 5 placebo-controlled C och rane,Psyclit quality usingJadad trials ofcyclobenz aprine scale,efficacy and with 312 patients,longest safety outcomes 24 weeks Skeletal Muscle Relaxants Page 89 of 237 Final Report Update 2 Drug Effectiveness Review Project Evidence Table 2. Tofferi L ow back painpatients, O verallquality ofstudies fair,with average quality N otassessed. Sleepimproved similarly incyclobenz aprine and placebo patients. Painimproved incyclobenz aprine patients atweek 4 only (SM D0. N o improvements infatigue ortenderpoints in cyclobenz arpine orplacebo groups. Skeletal Muscle Relaxants Page 90 of 237 Final Report Update 2 Drug Effectiveness Review Project Evidence Table 2. Included system aticreviews and m eta-analyses ofskeletalm uscle relaxants inpatients with m usculoskeletal conditions Tim e period covered and F unding A uth or sources used inliterature source and M eth od of C h aracteristics of Y ear A im s search Eligibility criteria Exclusioncriteria role appraisal identified articles VanTulder Systematicreview of th rough O ctober2001 R andomiz ed Studies of U niversity of Independently 27 studies excluded 48, 49 effectiveness of (M EDL IN E,EM BA SE)or controlled trials and ch lormez anone Toronto and assessed by two 2003 skeletalmuscle 2002 (C och rane L ibrary) double-blind and botulinum VU U niversity reviewers using 30 trials of2884 patients relaxants inth e controlled clinical toxin M edical criteria (11-item included (14 ofth ese treatmentofback M EDL IN E,C och rane L ibrary, trials ofpatients with C enter instrument) studies did notmeetour pain EM BA SE nonspecificlow back A msterdam recommended by inclusioncriteria because painreceiving th e C och rane Back th ey were non-English or skeletalmuscle R eview G roup. Included system aticreviews and m eta-analyses ofskeletalm uscle relaxants inpatients with m usculoskeletal conditions A uth or Population Y ear ch aracteristics M ainR esults A dverse events Internalvalidity VanTulder A cute orch roniclow A llstudies h ad atleasttwo criteria forwh ich itwas N onbenz odiaz epines versus placebo G O O D. M eanquality score 6 (range 3- (11 studies,pooled relative risks) 2003 degrees;age,race and 9,scale 0-11). Skeletal Muscle Relaxants Page 92 of 237 Final Report Update 2 Drug Effectiveness Review Project Evidence Table 2. Included system aticreviews and m eta-analyses ofskeletalm uscle relaxants inpatients with m usculoskeletal conditions Tim e period covered and F unding A uth or sources used inliterature source and M eth od of C h aracteristics of Y ear A im s search Eligibility criteria Exclusioncriteria role appraisal identified articles M eta-analysis N ibbelink A ssess th e Time period covered not C ontrolled clinical Studies outside A uth ors N otreported 20 double-blind 70 th erapeutic clear studies ofpatients th e U nited States employed by randomiz ed trials of1153 1978 response of with skeletalmuscle (3 studies) M erck. N ot patients (434 cyclobenz aprine N otclearwh atmeth ods used spasm treated with because of reported if cyclobenz aprine,280 compared to to identify relevantstudies, cyclobenz aprine, differences in funderh eld diaz epam,439 placebo) diaz epam and butappears to include diaz epam,or protocoland data data. Skeletal Muscle Relaxants Page 93 of 237 Final Report Update 2 Drug Effectiveness Review Project Evidence Table 2. N o evaluationfor 70 14% musculoskeletal G lobalresponse: C yclobenz aprine and diaz epam placebo h eterogeneity. Insufficientdetailof 1978 strain,10% idiopath ic, significantly betterth anplacebo,no significant Drowsiness: 39% vs. N otclearif 8% postoperative,6% differences betweencyclobenz aprine and Dry mouth : 24% vs. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity W ith drawals Type of Interventions Screened orlostto A uth or Study, Dose Exclusion Eligible follow-up Y ear Setting Duration Eligibility C riteria C riteria Enrolled A nalyz ed PopulationC h aracteristics Bass R andomiz ed A : Tiz anidine titrated to Patients with N otreported N otreported 18 with drew or Initialintervention: Tiz anidine vs. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or M eth od ofO utcom e A ssessm entand Y ear Tim ing ofA ssessm ent O verallR ating O utcom es Bass Spasms: 6 pointordinalscale F A IR. Durationofcontractures: N o significantdifferences between M uscle strength : N otclearh ow rated treatments C lonus: N otclearh ow rated R esolutionofclonus: 14/29 (48% )vs. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or F unding Source and Y ear A dverse events R ole O th ercom m ents Bass Tiz anidine vs. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity W ith drawals Type of Interventions Screened orlostto A uth or Study, Dose Exclusion Eligible follow-up Y ear Setting Duration Eligibility C riteria C riteria Enrolled A nalyz ed PopulationC h aracteristics C artlidge R andomiz ed A : Baclofen30 mg/day Spasticity,oth er N otreported N otreported 3 A ge range (years): 22-61 79 crossovertrial for2 weeks and 60 eligibility criteria F emale gender: 19/40 1974 mg/day for2 weeks unclear N otreported 37 R ace: N otreported U. B: Diaz epam 15 40 U nderlyingconditionmultiple sclerosis: 34/40 Single center mg/day for2 weeks and Baseline A sh worth score 3 or4 inatleast1 30 mg/day for2 weeks lowerlimb Priormuscle relaxantuse: N otreported 4 weeks intervention,4 weeks crossover C orston R andomiz ed A : Tiz anidine upto 24 Patients with N otreported N otreported 0/10 (0% ) Tiz anidine vs. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or M eth od ofO utcom e A ssessm entand Y ear Tim ing ofA ssessm ent O verallR ating O utcom es C artlidge Spasticity: A sh worth scale F A IR. U rinary frequency (improvementinpooled scores): +2 vs. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or F unding Source and Y ear A dverse events R ole O th ercom m ents C artlidge Baclofenvs. Skeletal Muscle Relaxants Page 100 of 237 Final Report Update 2 Drug Effectiveness Review Project Evidence Table 3. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity W ith drawals Type of Interventions Screened orlostto A uth or Study, Dose Exclusion Eligible follow-up Y ear Setting Duration Eligibility C riteria C riteria Enrolled A nalyz ed PopulationC h aracteristics Eyssette R andomiz ed A : Tiz anidine titrated to Patients age 18-70 N otreported N otreported 14/100 (14% ) Tiz anidine vs. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or M eth od ofO utcom e A ssessm entand Y ear Tim ing ofA ssessm ent O verallR ating O utcom es Eyssette Spasticity: 1 (absent)to 5 (spontaneous) F A IR. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or F unding Source and Y ear A dverse events R ole O th ercom m ents Eyssette F requentside effects: N otreported 73% ofpatients onbaclofen 73 Tiz anidine (n=50): 15 drowsiness,14 dry mouth ,8 fatigue,6 orth ostatich ypotension,7 insomnia priorto study entry, 1988 Baclofen(n=50): 10 drowsiness,12 fatigue,10 muscularweakness,9 disturbance ofaffect,8 proportionineach vomiting interventiongroupnot reported. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity W ith drawals Type of Interventions Screened orlostto A uth or Study, Dose Exclusion Eligible follow-up Y ear Setting Duration Eligibility C riteria C riteria Enrolled A nalyz ed PopulationC h aracteristics G lass R andomiz ed A : Dantrolene 100 mg N otreported N otreported N otreported 5 with drew Demograph ics notreported 82 crossovertrial qid 1974 62 11 C linicalconditions ofpatients enrolled not U. Inpatients eligible,39% C VA ,18% 16 spinalcord injury,12% M S,4% C P,4% Single center C : Dantrolene 100 mg miscellaneous (proportions notreported for qid + diaz epam 5 mg each interventiongroup) qid D: Placebo 4 2-week intervention periods H oogstraten R andomiz ed A : Tiz anidine titrated, M ultiple sclerosis Severe cardiac N otreported 5 Baseline ch aracteristics notreported foreach 74 trial range 12-24 mg/day patients with stable insufficiency, interventiongroup 1988 C rossover spasticity for>2 diastolicblood N otreported 14 M eanage (years): 55 B: Baclofentitrated, month s,K urtz ke pressure >110, F emale gender: 6/16 N eth erlands range 15-60 mg/day expanded disability severe 16 R ace: N otreported status score 4-7 h ypotension, Single center 2-3 weeks titration ch ronic A verage K urtz ke EDSS score:6. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or M eth od ofO utcom e A ssessm entand Y ear Tim ing ofA ssessm ent O verallR ating O utcom es G lass R esistance to passive stretch : 1-6 scale F A IR. A mbulation: A mbulationIndex interventiongroups Spasticity/tone: A sh worth scale,patient self-report(0-5 scale) R eflexes/clonus M uscle strength Efficacy: -3 to +3 scale Tolerance: -3 to +3 scale Skeletal Muscle Relaxants Page 105 of 237 Final Report Update 2 Drug Effectiveness Review Project Evidence Table 3. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or F unding Source and Y ear A dverse events R ole O th ercom m ents G lass W ith drawal(adverse event): 3/16 vs. N ot clearwh y 46/62 eligible patients were notentered into study. N otclearif patients wh o with drew from one interventionreceived oth erinterventions. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity W ith drawals Type of Interventions Screened orlostto A uth or Study, Dose Exclusion Eligible follow-up Y ear Setting Duration Eligibility C riteria C riteria Enrolled A nalyz ed PopulationC h aracteristics M edici R andomiz ed A : Tiz anidine titrated, O utpatients with H eartdisease, N otreported 2 death s and 3 Tiz anidine vs. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or M eth od ofO utcom e A ssessm entand Y ear Tim ing ofA ssessm ent O verallR ating O utcom es M edici N eurologicexam: K urtz ke meth od F A IR. F unctionalassessmentofdisability: 43% Pedersenscale Patientglobalassessmentofclinicalch anges: N o significant Patientself-assessmentofdisability: M ild, differences betweeninterventions (raw data notreported) moderate,severe,very severe Ph ysicianglobalassessmentofclinicalch anges: N o significant Ph ysicianglobalassessmentofclinical differences betweeninterventions (raw data notreported) ch anges:W orse,no ch ange,improvement, G lobalassessment/ph ysician(good to excellent):60% vs. H ead-to-h ead trials ofskeletalm uscle relaxants inpatients with spasticity A uth or F unding Source and Y ear A dverse events R ole O th ercom m ents M edici Tiz anidine vs.
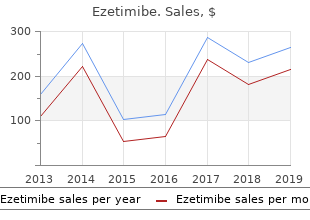
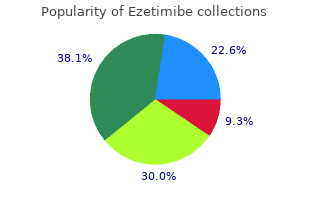
Purchase ezetimibe 10mg otc. 10 Fruits For High Cholesterol - Foods That Reduce Cholesterol.