
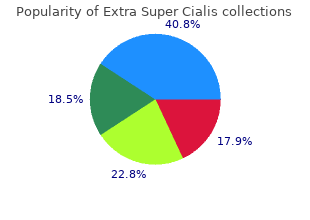
Mount Union College. G. Deckard, MD: "Purchase Extra Super Cialis - Best Extra Super Cialis".
Synergistic effects with benzodiazepines warrant close observation when this combination is given in the preoperative period purchase generic extra super cialis canada erectile dysfunction rings for pump. Figure 23-5 Percentage of patients in each group failing to recall specific events of the operative day buy generic extra super cialis line free erectile dysfunction drugs. There should be an attempt to maintain opioid use at the usual level by continuing methadone or substituting other appropriate agents for methadone extra super cialis 100 mg mastercard std that causes erectile dysfunction. The anesthesiologist should be cautioned about using agonist–antagonist drugs in these patients for fear of producing withdrawal. Anticholinergics Historically, anticholinergic drugs were widely used when inhalation anesthetics produced copious respiratory tract secretions and intraoperative bradycardia was a frequent danger. The advent of newer inhalation agents has markedly decreased the routine use of anticholinergic drugs for preoperative medication. Specific indications for an anticholinergic before surgery are (1) antisialagogue effect, (2) sedation and amnesia, and (3) vagolytic effect (Table 23-17). In the past, anticholinergics were also administered in an attempt to decrease gastric acid secretion, but research has shown them not to be effective for this purpose. For example, when awake fiberoptic tracheal intubation or bronchoscopic examination is planned, conditions will be more satisfactory for visualization when an anticholinergic drug has been administered. Glycopyrrolate is the most potent antisialagogue, with less likelihood of increasing heart rate than atropine. Because glycopyrrolate is a quaternary amine, it does not easily cross the blood–brain barrier and does not produce sedation or amnesia as seen with scopolamine, a tertiary amine. Table 23-17 Comparison of Effects of Three Anticholinergic Drugs 1534 Sedation and Amnesia Although midazolam has largely taken over as the preoperative sedative of choice, historically, scopolamine was often given intramuscularly in combination with an opioid. Scopolamine does not produce amnesia in all patients, and may not be as effective as lorazepam or diazepam in preventing recall. The additive amnestic effect may be useful for the unstable patient who does not tolerate general anesthesia; however, scopolamine is currently largely unavailable in the United States. Vagolytic Action Vagolytic action of the anticholinergic drugs is produced through the blockade of acetylcholine at the sinoatrial node. Atropine given intravenously is more potent than glycopyrrolate in increasing heart rate. The vagolytic action of the anticholinergic drugs is useful in the prevention of reflex bradycardia that may result from traction on extraocular muscles or abdominal viscera, carotid sinus stimulation, or repeated doses of succinylcholine. As these bradycardic events occur intraoperatively, it is more effective to administer the drug during anesthesia. Side Effects of Anticholinergic Drugs Central Nervous System Toxicity Scopolamine and atropine (tertiary amines) may cause central nervous system toxicity, the so-called central anticholinergic syndrome. This syndrome is most likely to occur after the administration of scopolamine, but can be seen after high doses of atropine and may include symptoms such as delirium, restlessness, confusion, and obtundation. Elderly patients and patients with pain appear to be particularly susceptible; the syndrome has been noted to be potentiated by inhalation anesthetics. The administration of 1 to 2 mg of physostigmine intravenously can successfully treat the syndrome. Intraocular Pressure Mydriasis and cycloplegia from anticholinergic drugs may place patients with glaucoma at risk for increased intraocular pressure. Atropine and glycopyrrolate may be less likely to increase intraocular pressure than scopolamine. In patients with glaucoma, it is generally safe to continue most glaucoma medications up until the time of surgery or use atropine or glycopyrrolate when necessary. Hyperthermia 1535 Sweat glands of the body are innervated by the sympathetic nervous system, but use cholinergic transmission. Antibiotic Prophylaxis Surgical antibiotic prophylaxis has become an outcome measure on which hospital and anesthesia performance is measured. Reimbursement or even accreditation may depend on properly timed and dosed administration. Anesthesiologists frequently administer antibiotics to patients prior to surgery for contaminated and clean-contaminated procedures or for clean surgical procedures when infection would be catastrophic, such as for device implants. Other indications for the use of prophylactic antibiotics include the prevention of endocarditis and the prevention of infection in immunocompromised patients. Cephalosporins are the most popular antibiotics because they cover common skin microbes. The National Surgical Infection Project recommends that antibiotics be administered within 1 hour prior to incision. Furthermore, if the surgical procedure is prolonged, it is recommended that the antibiotic be redosed when two half-lives have elapsed. For example, cefazolin has a half- life of 2 hours; therefore, it should be redosed if the surgical procedure extends past 4 hours. Research on morbidly obese patients has shown that the dose required to achieve adequate tissue levels is twice that for normal- weight patients. Summary of Patient Preparation The anesthesiologist who takes the time to adequately prepare the patient medically and psychologically for anesthesia and surgery will find that his/her job of caring for the patient intraoperatively becomes easier, and is more likely to have both a positive clinical outcome and a satisfied patient. Practice advisory for preanesthesia evaluation: An updated report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. The Perioperative Surgical Home, A Comprehensive Literature Review for the American Society of Anesthesiologists. The preoperative evaluation form: Assessment of quality from one hundred thirty-eight institutions and recommendations for a high-quality form. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. The development and validation of a risk score to predict the probability of postoperative vomiting in pediatric patients. Angina and other risk factors in patients with cardiac diseases undergoing noncardiac operations. Prevention of infective endocarditis: Guidelines from the American Heart Association: A Guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Hospital admission blood pressure, a predictor for hypertension following endotracheal intubation. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Development and validation of a risk calculator for prediction of cardiac risk after surgery. Is a pre-operative brain natriuretic peptide or N-terminal pro-B-type natriuretic peptide measurement an independent predictor of adverse cardiovascular outcomes within 30 days of noncardiac surgery? Prognostic value of brain natriuretic peptide in noncardiac surgery: A meta-analysis. The predictive ability of preoperative B- type natriuretic peptide in vascular patients for major adverse cardiac events. Perioperative outcome and long- term mortality for heart failure patients undergoing intermediate and high-risk noncardiac surgery: Impact of left ventricular ejection fraction. Prognostic implications of asymptomatic left ventricular dysfunction in patients undergoing vascular surgery. Reevaluation of perioperative myocardial infarction in patients with prior myocardial infarction undergoing noncardiac operations.
Eur J Cardiothorac Surg 49: fulminant myocarditis in adult patients: a 5-year multi- 73–77 institutional experience buy extra super cialis 100mg line erectile dysfunction books download free. J Am Coll Cardiol circulatory support for fulminant myocarditis 61(3):313–321 complicated by cardiogenic shock buy extra super cialis cheap erectile dysfunction medication ratings. Saito S trusted extra super cialis 100 mg erectile dysfunction otc meds, Matsumiya G, Sakaguchi T, Miyagawa S, Naka Y (2005) Left ventricular assist device Yoshikawa Y, Yamauchi T et al (2010) Risk factor implantation after acute anterior wall myocardial analysis of long-term support with left ventricular infarction and cardiogenic shock: a two-center study. Circ J 76:1631–1638 139:1316–1324 121 11 Bridge to Transplant and Destination Therapy Strategies in the United States Yasuhiro Shudo, Hanjay Wang, Andrew B. Decisions about candidacy heart transplantation and have no absolute for each strategy should be made collaboratively contraindications to transplant, but who have by an experienced heart failure team, including medical, social, or fnancial barriers to transplant both surgeons and cardiologists, and reassessed as candidacy at the time of evaluation) and bridge to dictated by the patient’s clinical course. A thorough listed for heart transplant at the time of device assessment of operative risk and potential implantation. Tus, for end- therapy, the overall operative risk combines stage heart failure patients with contraindications those associated with two surgeries instead of to heart transplantation, commonly including one. Tese operation would involve a redo sternotomy and patients also experience signifcant improvements repeat cardiopulmonary bypass, both of which in quality of life based on assessments such as the are associated with increased operative risk. As introduced are less ill and who have not yet developed sequelae previously, the prospectively randomized of end-stage cardiac insufciency. Te pump can generate Support fows up to 10 L/min, operating at pump speeds of 6,000 rpm to 15,000 rpm. Patient-specifc durability of the pump and also allow for a factors that should be considered include the reduction in the size and weight of the device. For right but in the absence of treatment, mortality within ventricular support, the right atrium and 6 months was 48%. With a total displaced volume is compatible with patients of almost any body of 50 mL and weight of 160 g, the HeartWare size. Using a transplanted patients surviving to hospital magnetically and hydrodynamically levitated discharge [21]. Te replacement biventricular support had survival- to- of mechanical bearings by the frictionless, transplantation rates of 41% and 55%, respectively. Te device consists of a 65 mL stroke eliminates any other abnormalities of the native volume pump placed in a paracorporeal position heart, including valve dysfunction and outside of the body on the abdomen anteriorly, arrhythmias. Te device weighs 200 g and is randomized study of 200 transplant-ineligible implanted into the pericardial space. A continuation 10 L/min and also features pump speed of this study more recently demonstrated modulation, allowing for antithrombotic cycling updated 1- and 2-year survival rates to be 73% to prevent thrombosis of the pump. Anand I, Maggioni A, Burton P et al (2006) The seattle decade, signifcant progress has been made with heart failure model: prediction of survival in heart regard to patient selection and management, failure. J Thorac challenge heart transplantation as the standard of Cardiovasc Surg 137(4):971–977 care for advanced heart failure. Mancini D, Lietz K (2010) Selection of cardiac management of chronic heart failure in the adult: a transplantation candidates in 2010. Circulation report of the American College of Cardiology/ 122(2):173–183 Review American Heart Association Task Force on Practice 16. N Engl J Med 370(1):33–40 with a continuous fow left ventricular assist device as a 20. Presented at the International Society for Recommendations for the use of mechanical Heart and Lung Transplantation 35th Annual Meeting circulatory support: device strategies and patient and Scientifc Sessions, 15–18 Apr, Nice 131 12 Mechanical Circulatory Support as Bridge to Recovery Michael Dandel and Stephan Schueler 12. Myocardial recovery in recurred in about one half of them during the patients who were successfully weaned from first 10 post-weaning years. In weaned patients “recovery” with freedom from future heart with nonischemic cardiomyopathy as the events. However, improvement in myocyte contraction and the few studies on reverse remodeling at cellular relaxation [6, 10, 12]. In a study (synthetic thrombin inhibitor) infusions (2 μg/kg/ which compared long-term outcomes of patients min started 1 h before of-pump trials) [22]. Before the which might interfere with possibly still ongoing frst of-pump trial, it is useful to perform stepwise recovery. Tus, if underwent assessments of cardiac recovery incomplete interruption of unloading already exclusively at rest [9, 22]. If the patient remains asymptomatic but adaptation to stress, the weaning results appeared. Te same the risk of myocardial exhaustion with negative group also uses cardiopulmonary exercise impact on an ongoing myocardial recovery process. However, in border- explant cardiac stability of ≥10 years can reach line cases, of-pump data on deformation velocity 90%. Exercise testing also appeared as well as on intraventricular synchrony and predictive for recovery. Unfortunately the low rates of 143 12 Mechanical Circulatory Support as Bridge to Recovery. Te possible superiority of strain imaging in this Recovery occurred more ofen in patients matter needs to be assessed in the future. What causes the great discrepancy between cardiac recovery under mechanical the high recovery rates on cellular and unloading? Image (d) also shows a normalization of early/late longitudinal strain (myocardial longitudinal shortening) diastolic strain rate ratio 146 M. Hetzer R, Müller J, Weng Y, Wallukat G, Spiegelsberger ventricular assist devices to the recovery of failing S, Loebe M (1999) Cardiac recovery in dilated hearts: a review and the Berlin Heart Centert cardiomyopathy by unloading with a left ventricular Experience. A companion to genomic and functional changes that occur in the braunwald’s heart disease. Elsevier, Philadelphia, failing heart in response to mechanical circulatory pp 258–271 support. Elsevier, Philadelphia, pp 258–271 of patients bridged to recovery versus patients 15. Hetzer R, Müller J, Weng Y, Meyer R, Dandel M myocardium after prolonged left-ventricular mechanical (2001) Bridging-to-recovery. J Heart Lung Transpl 28(7):710–717 pulsatile left ventricular assist devices than with 18. Ann Thorac Surg Winterfeld M, Takeda A, Takeda N, Stypmann J, 91(5):1335–1340 Vahlhaus C, Schmid C, Pomjanski N, Böcking A, Baba 30. Muranaka H, Marui A, Tsukashita M, Wang J, Nakano J, Cardiovasc Surg 141:616–623 Ikeda T, Sakata R (2010) Prolonged mechanical 31. J Card Fail 16(2):99–105 149 13 Mechanical Circulatory Support as Bridge to Candidacy Maria Frigerio, Manlio Cipriani, and David Feldman 13. In most cases, at least partial improvement mid- to long-term support may be useful to of the hemodynamic profle may be obtained with allow desensitization and/or to wait for a pharmacological therapy, but especially when it is compatible donor. Obser- associated with a reduced risk of developing 13 vational experiences in a limited number of cases malignancies and a reduced speed of their pro- appear to obtain some additional hemodynamic gression [25–27]. Tus, a situation neoplastic drugs and/or radiotherapy that may in which the interests of individuals and of the have caused heart disease or at least contributed community could collide, which 10 years ago had to it. Post-chemotherapy cardiomyopathy is not been debated as a theoretical case, may be now a rarely characterized by biventricular compromise real clinical and ethical dilemma [39]. Moreover, chest radiotherapy In any case, expectations and uncertainties should may damage the heart via several mechanisms, be explained with realism and frankness to the including valvular disease, pericardial thickening patients and their families.
Peripheral vasoconstriction buy extra super cialis 100mg mastercard erectile dysfunction drugs for sale, which results from central sympathetic control of subcutaneous vascular tone discount extra super cialis 100 mg amex erectile dysfunction doctor in los angeles, is probably the most frequent and clinically the most important impediment to wound oxygenation and wound healing order generic extra super cialis erectile dysfunction medications generic. All vasoconstrictive stimuli must be corrected simultaneously to allow optimal healing. Modifiable risks for wound infections include smoking, malnutrition, obesity, hyperglycemia, hypercholesterolemia, and hypertension. Maintenance of a high room temperature or active warming before, during, and after the operation is significantly more effective than other methods of warming, such as application of warmed blankets, circulating water blankets placed on the surface of the operating table, and humidification of the breathing circuit. Current best recommendations for volume management include replacing fluid losses based on standard recommendations for the type of surgery, replacement of blood loss, and replacement of other ongoing fluid losses (e. Pain control also appears important since it favorably influences both pulmonary function and vascular tone. Wound complications are associated with2 prolonged hospitalization, increased resource consumption, and even increased mortality. A growing body of literature supports the concept that patient factors are a major determinant of wound outcome following surgery. Comorbidities such as diabetes and cardiac disease clearly contribute, and a patient’s genetic make-up may also contribute. Environmental stressors and3 the individual response to stress are also important. In particular, wounds are exquisitely sensitive to hypoxia, which is both common and preventable. Perioperative management can be adapted to promote postoperative wound healing and resistance to infection. Along with aseptic technique and prophylactic antibiotics, maintaining perfusion and oxygenation of the wound is paramount. This chapter discusses how knowledge of the principles of infection control and the biology and physiology of wound repair and resistance to infection can improve outcomes. The graph shows the distribution of adverse events within the subcategory of operative care (7,716 operative adverse events). In 1847, Ignaz Semmelweis made the observation that women who delivered their babies in the First Clinic at the General Hospital of Vienna, staffed by medical students and physicians, had a mortality rate of 5% to 15%, largely the result of puerperal infections; this was substantially higher than the 2% rate of women who delivered at Clinic 2, which was staffed by midwife students and midwives. Students and physicians at Clinic4 1 usually started the day performing autopsies (including on patients who died of puerperal fever) and then moved on to the clinic, where they performed examinations on women in labor. Semmelweis made the connection, and although germ theory was some years off, he insisted that physicians and medical students wash their hands in a chlorinated solution when leaving the pathology laboratory. Soon, Semmelweis identified cases of transmission from an infected to an uninfected patient, and instituted the use of chlorinated solution hand washing between cases as well. He also demonstrated that the chlorinated solution was more effective than soap and water. Unfortunately, his innovation was not widely adopted, resulting from a combination of his delay in publishing his results, the reluctance of his colleagues to accept that they might be responsible for transmitting disease, and his lack of tact in trying to convince health-care workers to adopt his measures. Transient flora colonize the superficial layers of the skin and thus are easier to remove with hand hygiene. Transient flora are also the source of most health-care–associated infections, as health-care worker skin can become contaminated from patient contact or contact with contaminated surfaces. Contamination from surfaces is 504 most commonly with organisms such as Staphylococci and Enterococci, which are resistant to drying. Even “clean” activities such as taking a patient’s pulse or applying monitors can lead to hand contamination: 100 to 1,000 colony- forming units of Klebsiella species were measured on nurses’ hands following such activities in one study. No studies have related hand contamination to7 actual transmission of infection to patients; however, numerous studies, starting with those of Semmelweis, have demonstrated a reduction in health- care–associated infections following institution of hand hygiene or improved adherence to hand hygiene. The ideal agent kills a broad spectrum of microbes, has antimicrobial activity that persists for at least 6 hours after application, is simple to use, and has few side effects. Plain (not antiseptic) soap and water are generally the least effective at reducing hand contamination. Although obvious dirt is removed by the8 detergent effect of soap and the mechanical action of washing, bacterial load is not greatly reduced. Further, soap and water hand hygiene is associated with high rates of skin irritation and drying, both of which are risk factors for an increased bacterial load. Soap and water are, however, the most effective at removing spores, and therefore should be used when contamination with Clostridium difficile or Bacillus anthracis is a concern. Ethanol is most commonly used because it has6 more antiviral activity than isopropanol. Antiseptics containing 60% to 95% ethanol with a water base are germicidal and effective against gram-positive and gram-negative bacteria, lipophilic viruses such as herpes simplex, human immunodeficiency, influenza, respiratory syncytial, and vaccinia viruses, and hepatitis B and C viruses. They have little persistent activity, although regrowth of bacteria does occur slowly after use of alcohol-based products. Combination with low doses of other agents such as chlorhexidine, quaternary ammonium compounds, or triclosan can confer persistent activity. Efficacy depends on volume applied (3 mL is superior to 1 mL) and duration of contact (ideally, 30 seconds). It is germicidal6 against gram-positive bacteria and lipophilic viruses, with somewhat less activity against gram-negative bacteria and fungi, and minimal against tubercle bacilli. It may cause severe corneal damage after direct contact with the eye, ototoxicity after direct contact with the inner or middle ear, and neurotoxicity after direct contact with the brain or meninges. There are reports of bacteria that have acquired reduced susceptibility to chlorhexidine, but these are of questionable clinical 506 pertinence since the concentrations at which resistance was found were substantially lower than that of commercially available products. Recent reports have identified immunoglobulin E–mediated allergic reactions to chlorhexidine. Cases are likely underreported because of the difficulty9 identifying the source of anaphylactic reactions perioperatively. Chlorhexidine is present in a wide range of medical and community-based products, including wipes, impregnated central venous catheters, toothpaste, mouthwash, contact lens cleanser, and food preservatives. Table 8-2 Indications for Hand Hygiene Iodine and iodophors (iodine with a polymer carrier) penetrate the cell wall and impair protein synthesis and cell membrane function. They are6 bactericidal against gram-positive, gram-negative, and some spore-forming bacteria including clostridia and Bacillus species, although inactive against spores. They cause more contact dermatitis than other commonly used agents, and allergies to this class of topical agent are common. The choice of an antiseptic depends on the expected pathogens, acceptability by health-care workers, and cost. In general, antiseptics cost about $1 per patient day, far less than the cost of health-care–associated infections. In nine studies that examined the effect of improved hand hygiene adherence on health-care–associated infections, the majority demonstrated that as hand hygiene practices improved, infection rates decreased. Although alcohol-based agents have long been believed to cause more skin irritation, several recent trials have demonstrated less skin irritation and better acceptance with emollient-containing, alcohol- based hand rubs compared with either antimicrobial or nonantimicrobial soaps. The use of appropriate (glove-compatible) lotions twice a day also reduces skin irritation—as well as leading to a 50% increase in hand hygiene frequency in one study. Alcohol-based gels and foams are also generally6 more accessible than antiseptic soap and water, as the dispenser may be pocket-sized or placed conveniently near sites of patient care. It has been estimated that alcohol-based gels and foams require only about 25% of the time of going to a sink to wash one’s hands.
Cell salvage in hip and knee arthroplasty: A meta-analysis of randomized controlled trials discount extra super cialis 100 mg fast delivery erectile dysfunction medicine reviews. Impaired red blood cell deformability after transfusion of stored allogeneic blood but not autologous salvaged blood in cardiac surgery patients cheap extra super cialis 100 mg fast delivery erectile dysfunction over 60. Laboratory characteristics and clinical utility of post-operative cell salvage: washed or unwashed blood transfusion? Additional postoperative cell salvage of shed mediastinal blood in cardiac surgery does not reduce allogeneic blood transfusions: a cohort study purchase extra super cialis 100mg fast delivery erectile dysfunction prevents ejaculation in most cases. Inherited disorders of platelet function 1178 and challenges to diagnosis of mucocutaneous bleeding. Evaluation of a von Willebrand factor three test panel and chemiluminescent-based assay system for identification of, and therapy monitoring in, von Willebrand disease. Achievements, challenges and unmet needs for haemophilia patients with inhibitors: Report from a symposium in Paris, France on 20 November 2014. The realm of vitamin K dependent proteins: shifting from coagulation toward calcification. Guideline for reversal of antithrombotics in intracranial hemorrhage: A statement for healthcare professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Guidelines for the diagnosis and management of disseminated intravascular coagulation. Cyclooxygenase-2 inhibitors, nonsteroidal anti- inflammatory drugs, and cardiovascular risk. Cardiovascular disease and non-steroidal anti-inflammatory drug prescribing in the midst of evolving guidelines. Laboratory evaluation of clopidogrel responsiveness by platelet function and genetic methods. Recent progress in anticoagulant therapy: oral direct inhibitors of thrombin and factor Xa. Direct-acting oral anticoagulants: pharmacology, indications, management, and future perspectives. Comparison of the efficacy and safety 1180 of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta- analysis of randomised trials. The use of novel oral anticoagulants for thromboprophylaxis after elective major orthopedic surgery. Desmopressin reduces transfusion needs after surgery: a meta-analysis of randomized clinical trials. Solubility alone determines the rate of elimination, provided there is normal cardiopulmonary function. Concentrations of inhaled anesthetics that provide loss of awareness and recall are about 0. The latter effect may increase intracranial pressure in patients with a mass-occupying lesion of the brain. Introduction and Overview Inhalation anesthetics are the most common drugs used for the provision of general anesthesia. Adding only a fraction of a volatile anesthetic to the inspired oxygen results in a state of unconsciousness and amnesia. When combined with intravenous adjuvants, such as opioids and benzodiazepines, a balanced technique is achieved that results in analgesia, further sedation/hypnosis, and amnesia. Inhaled anesthetics for surgical procedures are popular because of their ease of administration and the clinician’s ability to reliably monitor their effects with both clinical signs and end-tidal concentrations. In addition, the volatile anesthetic gases are relatively inexpensive in terms of overall cost. Sevoflurane, desflurane, and isoflurane are the most popular potent 1184 inhaled anesthetics used in adult surgical procedures (Fig. Although there are many similarities in terms of the overall effects of the volatile anesthetics (e. For example, sevoflurane is the most commonly used anesthetic in the pediatric population based on its relative lack of pungency when inhaled and its relative speed of emergence. These beneficial attributes outweigh the emergence agitation associated with the use of sevoflurane in pediatric patients. Discussion of the attributes of the three most popular inhaled anesthetics provides the major emphasis of this chapter. For the sake of completeness and for historical perspective related to metabolism and toxicity, comments on halothane and enflurane are also included. Desflurane differs from isoflurane in the substitution of a fluorine for a chlorine atom and sevoflurane is a methyl isopropyl ether. Pharmacokinetic Principles Kety in 1950 was the first to examine the pharmacokinetics of inhaled agents1 in a systematic fashion. Eger accomplished much of the early research in the2 field, leading to his landmark text on the subject in 1974. The inhaled anesthetics differ substantially from nearly all other therapeutic drugs because they are gases given via inhalation. Drug pharmacology is classically divided 1185 into two disciplines, pharmacodynamics and pharmacokinetics. It describes the desired and undesired effects of drugs, as well as the cellular and molecular changes leading to these effects. It describes where drugs are distributed, how they are transformed, and the cellular and molecular mechanisms underlying these processes. An important implication of different compartments and perfusion rates is the concept of redistribution. After a given amount of drug is administered, it reaches highly perfused tissue compartments first, where it can equilibrate rapidly and exert its effects. With time, however, compartments with lower perfusion rates receive sufficient drug to reach equilibrium between blood and tissue. As the tissues with lower perfusion rates absorb the drug, maintenance of equilibria throughout the body requires drug transfer from highly perfused compartments back into the bloodstream. This lowering of drug concentration in one compartment by delivery into another compartment is called redistribution. In discussions of the inhaled anesthetics, the absorption phase is usually called uptake, the metabolic phase is usually called biotransformation, and the excretion phase is usually called elimination. Unique Features of Inhaled Anesthetics Speed, Gas State, and Route of Administration The inhaled anesthetics are among the most rapidly acting drugs in existence, and when used for general anesthesia, this speed provides a margin of safety. The ability to quickly increase or decrease anesthetic levels as necessary can mean the difference between an anesthetic state and an anesthetic misadventure. Rapid induction and recovery may lead to faster operating room turnover times, shorter recovery room stays, and earlier discharge times to home. Only N O and xenon are true gases, while the so-called2 potent anesthetics are the vapors of volatile liquids. But for simplicity, all of them are referred to as gases because they are all in the gas phase when administered via the lungs. This allows them to diffuse rapidly without the need for facilitated diffusion or active transport from bloodstream to tissues.
