
Lawrence Technological University. X. Hauke, MD: "Buy cheap Biaxin online - Effective Biaxin no RX".
Clinical pharmacy cardiac risk service for managing patients with coronary artery disease in a health maintenance organization purchase biaxin uk collagenous gastritis definition. Implementation of a quality assurance program to ensure the safety and effectiveness of a centralized pharmacy automation system order biaxin american express gastritis with chest pain. Telematics applications to support the role of the community pharmacists as self-medication advisors 500 mg biaxin fast delivery xanthomatous gastritis. A fuzzy logic-based decision support system on anesthetic depth control for helping anesthetists in surgeries. The development and impact of a drug exception reporting system in a psychiatric facility. A stepwise approach to the evaluation and selection of a hospital pharmacy information system. Introduction of an electronic charting software with computerized physician order entry and medication safety features - Experience at the University Hospital Freiburg, Germany. Development of a medication safety strategic plan for a hospital or health system. What evidence supports the use of computerized alerts and prompts to improve clinicians’ prescribing behavior? Strategy for implementation and first results of advanced clinical decision support in hospital pharmacy practice. Computerized prescribing: building the electronic infrastructure for better medication usage. Linking laboratory and pharmacy: opportunities for reducing errors and improving care. Effective change to the distribution process, which decreased medication turnaround time. Computer program to assist pharmacy management of an inpatient warfarin dosing service. Comparison of implementation of a physician order entry system in the inpatient and outpatient setting. Implementation of a closed loop verification program: Reporting problematic bar codes in a bar code medication administration system from the reporting facility to manufacturer notification. Personal health information management and the design of consumer health information technology: Secondary analysis of data from the medical expenditure panel survey. Derivation and cross-validation of pharmacokinetic parameters for computer-controlled infusion of lidocaine in pain therapy. Design and implementation of a web-based patient portal linked to an electronic health record designed to improve medication safety: the Patient Gateway medications module. A mobile-phone based teledermatology system to support self-management of patients suffering from psoriasis. Controlled study on the use of hand-held insulin dosage computers enabling conversion to and optimizing of meal-related insulin therapy regimens. Health Telematics - Current Developments and Consequences for Hospitals and Care-providers. Diabetes self-adjustment by a computerized program- first experiences in inpatient and outpatient treatment. Evaluation of documentation of patient height, weight, and allergy information at a university medical center. Design and acceptability of patient-oriented computerized diabetes care reminders for use at the point of care. Medication safety teams’ guided implementation of electronic medication administration records in five nursing homes. An empirical and policy analysis of the impact of Divisions within the Australian health care system. Achieving better in-hospital and after-hospital care of patients with acute cardiac disease. Early implementation experiences with an orders interface from a clinical information system to a pharmacy system: Challenges of blending two workflows. Impact of robotic technology on the accuracy and quality of a centralized cart fill process. Toward development of a computer-based methodology for evaluating and reducing medication administration errors. Antiretroviral drug interactions: often unrecognized, frequently unavoidable, sometimes unmanageable. Financial/workload evaluation for an automated controlled substance dispensing system. Implementation of a commercially available clinical decision support system to decrease adverse drug events: an exploratory descriptive analysis. Advances in Patient Safety: From Research to Implementation 2005;2: Concepts and Methodology: Grey Lit. Adverse drug event detection in a community hospital utilising computerised medication and laboratory data. Computer networking to enhance pharmacist-physician communication: A pilot demonstration project in community settings. Steps in multidisciplinary implementation of `smart pump” technology to optimize patient safety. Imputation of consumption to patient in three different clinical units with automated dispensing systems. Modeling patient-specific therapeutic strategy in the guideline-based management of a chronic disease. Reminder-based or on-demand decision support systems: a preliminary study in primary care with the management of hypertension. Computerized ambulatory care pharmacy information system for direct order entry by prescribers. Development of an electronic pharmacy patient profiling system in the era of computerized physician order entry. Wireless clinical alerts for critical medication, laboratory and physiologic data. Primary care physicians’ use of an electronic medical record system: a cognitive task analysis. Review of the evidence of the impact of computerized physician order entry system on medication errors. The development of a computerised equipment and drug calculator for use in resuscitation. HandiStroke: A handheld tool for the emergent evaluation of acute stroke patients. Understanding the impact on intensive care staff workflow due to the introduction of a critical care information system: a mixed methods research methodology. A Meta-analysis of 16 randomized controlled trials to evaluate computer-based clinical reminder systems for preventive care in the ambulatory setting. Past, present, and future of insulin pump therapy: A better shot at diabetes control. Comparison of the applicability of rule-based and self- organizing fuzzy logic controllers for sedation control of intracranial pressure pattern in a neurosurgical intensive care unit.
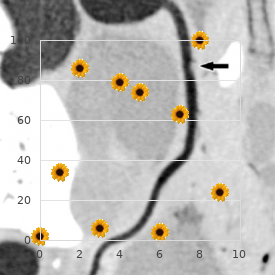
Various pharmacokinetic evaluations in humans biaxin 250mg with visa gastritis cystica profunda, including those illustrated in Figure 7 order cheap biaxin online gastritis treatment and diet. In contrast cheap 500mg biaxin free shipping chronic gastritis diet plan, transdermal delivery of melatonin results in a significant delay in systemic melatonin levels and a gradual decline in drug delivery after patch removal, possibly due to deposition of melatonin in the skin (Figure 7. Moreover, plasma levels tend to be lower after transdermal delivery and inter-subject variability to be higher. Pharmacokinetic evaluations comparing transmucosal, oral-controlled release and transdermal delivery of melatonin clearly demonstrated that the transmucosal route is the best dosage form to mimic endogenous secretion of this drug (Figure 7. Acceptability and compliance studies have shown that the patch is accepted favorably by patients. They are recommended for use in the post-operative prevention of thromboembolic disorders and are conventionally administered via the subcutaneous route. To maximize transmucosal absorption, the active was incorporated in a Cydot uni-directional reservoir system. Use of a reservoir system allows a high degree of drug loading and also permits absorption enhancers to be included with the drug in the central reservoir compartment. Studies have demonstrated that the patches: • possess prolonged adhesion properties; • are of low irritancy; • have bioavailabilites ranging from 50% to 75%. The TheraTech buccal delivery system comprises a bilayer tablet, with an adhesive layer on one side, and an active layer on the other side, which lies in contact with the cheek mucosa. However, the route is associated with many advantages for drug delivery and there is clearly considerable ongoing research in this area. In the past decade, new and highly sophisticated formulations have been developed; drug delivery using the new types of retentive systems for buccal absorption is a particularly promising area. Some success has also been attained in the transbuccal delivery of peptides and proteins. Thus it can be expected that a more exponential growth phase will develop in the coming years. Name 3 differences between the buccal mucosa and the mucosa of the gastrointestinal tract. What advantages does the buccal route offer for the systemic delivery of peptides? What is the main structural difference between the gingival and the cheek epithelium? Rank the permeability of the gastrointestinal mucosa, the skin and the buccal mucosa in the order lowest to highest. Evolution has provided the mammalian organism with an external covering, the principal function of which is to act as a barrier, specifically to the loss of tissue water. Think about it: the concentration of water inside the human body is 190 on the order of 50 M, while that in the atmosphere is clearly very much less. Thus, there is a strong driving force for water to be lost from the body and, to prevent desiccation, an efficient barrier at the interface is therefore required. The skin, and more specifically skin’s outermost layer, the stratum corneum, provides this shield. Of course, in so doing, the skin also presents a formidable resistance to the absorption, either deliberate or accidental, of chemicals which contact the external surface. Nevertheless, the challenge of transdermal drug delivery has been accepted by pharmaceutical scientists and, over the past 25 years, considerable progress and achievement have been recorded. So, what led to the investigation of the skin as a potential route for systemic drug input in light of the formidable challenges posed by the stratum corneum? First, the skin offers a large (1–2 m ) and very accessible surface for drug2 delivery. Second, transdermal applications, relative to other routes, are quite noninvasive, requiring the simple adhesion of a “patch” much like the application of a Band-Aid. As a result, thirdly, patient compliance is generally very good—that is, in general, people are quite comfortable with the use of a simple-looking patch (no matter how complex the interior machinery). And, fourth, with again a positive aspect for the patient, a transdermal system is easily removed either at the end of an application period, or in the case that continued delivery is contra-indicated—with the exception of intravenous infusions, no other delivery modality offers this advantage. Although transdermal administration is limited at present to relatively few drugs, it has proven to be a considerable commercial success when compared to other “controlled release” technologies. The current worldwide market for transdermal systems is about $2 billion annually. Macroscopically, skin comprises two main layers: the epidermis and the dermis (~0. The dermal-epidermal junction is highly convoluted ensuring a maximal contact area. Other anatomical features of the skin of interest are the appendageal structures: the hair follicles, nails and sweat glands. The keratinocytes comprise the major cellular component (>90%) and are responsible for the evolution of barrier function. The epidermis per se can be divided into five distinct strata which correspond to the consecutive steps of keratinocyte differentiation. The ultimate result of this differentiation process is formation of the functional barrier layer, the stratum corneum (~0. The stratum basale or basal layer is responsible for the continual renewal of the epidermis (a process occurring every 20–30 days). Proliferation of the stem cells in the stratum basale creates new keratinocytes which then push existing cells towards the surface. The next layer of the epidermis is the stratum spinosum, named for the numerous spiny projections (desmosomes) on the cell surface. The keratinocytes maintain a complete set of organelles and also include membrane-coating granules (or lamellar bodies) which originate in the Golgi. Subsequently, we encounter the stratum granulosum or granular layer, characterized by numerous keratohyalin granules present in the cytoplasm of the more flattened, yet still viable, keratinocytes. More lamellar bodies are also apparent and concentrate in the upper part of the granular cells. The transition layer, the stratum lucidum, comprises flattened cells which are not easy to visualize microscopically. The cellular organelles are broken down leaving only keratin filaments in the stratum granulosum an interfilament matrix material in the intracellular compartment. The membrane coating granules fuse with the cell membrane and release their contents into the intercellular space. Finally, in the stratum corneum, the outermost layer, protein is added to the inner surface of the cell membrane to form a cornified envelope that further strengthens the resistance of the cell. A layer of lipid covalently bound to the cornified envelope of the corneocyte contributes to this exquisite organization. The intercellular lipids of the stratum corneum include no phospholipids, comprising an approximately equimolar mixture of ceramides, cholesterol and free fatty acids.
Hospital administrators place emphasis on other aspects such as costs purchase generic biaxin from india gastritis diet of hope, return on investment buy generic biaxin pills gastritis keeps coming back, and organizational change purchase biaxin 500 mg on line gastritis uti. The relative importance of these factors will vary among physicians practicing in different settings, with cost being more important to physicians in private practice than in hospitals, and other related issues. Similarly, the importance of these factors will vary among pharmacists depending on their practice setting and the type of technology. Work needs to be done to identify the needed critical information before we can truly assess what is missing. From the information garnered in this report, a growing body of evidence supports the use of some technologies (e. Each of the 21 articles included in this section established 800 653,789,791,793,798 evidence on likelihood to use, one on purchase, and five on implementation. A sizeable number (n = 20) of articles were on the prescribing and ordering phases, with only one 45 on the administering phase of medication management. However, the literature is sparse and evidence from studies with stronger methods that can address this question is lacking. Fundamental issues related to system characteristics included the availability and accessibility of hardware, technical support and training, system integration into clinical workflow, timeliness of clinical messages, and acceptance of the system by various 803 stakeholders. Another review involving descriptions of 112 information systems identified that for successful implementation, core components were order entry, guideline adherence, and 804 decision support. Involving end users in the development process was also shown to be a key 804 to success. Nineteen 800 articles were published in the original literature and one was from the grey literature. More than half of the studies (n = 13) evaluated 661 667 physicians as the user of the technology. One study convened a panel of technical experts 801 representing organizations having direct experience in implementing e-Prescribing standards. In most of the studies, the participants were primarily from hospitals, 791,793 45 632,653,667,798-800 and some were set in pharmacies, ambulatory care, and primary 794,795,797 48,792,796,802 care. Research methods were weak: eighteen articles were surveys, two used 801,805 qualitative research, while one used data from scientific literature, organizations, 797 government, and professional reports. Bell and colleagues conducted an expert panel consensus that resulted in 60 specific functional recommendations for e-Prescribing to improve patients’ health 806 outcomes and reduce costs. List of articles addressing various features that were instrumental in the decision to purchase, implement, and use Features Number of Studies Addressing the Features 632,653,663,789,792,794,798,799,801 Medication list 9 661,789,792,793,799 eDosing calculations 5 45,632,653,661,667,789-794,796,798-801 Clinical decision support (alerts and messages 16 for allergies, drug-drug interaction, drug approval) 48,632,653,667,790,792,794-799,802 e-Prescribing 13 45,632,792,794,798 Order communication of prescription to 5 pharmacies 45,789,790,792,794,797,799,800,802 Access to laboratory test results 9 661,789,792,795,796,799 Implementation of guidelines 6 791 Transcription services 1 653,793,795,801 Formulary information 4 45 Tallman letters and change of color to 1 differentiate between look-alike drug name pairs, 45,791,793 Integration with another system (e. Wang and colleagues suggest that mandating the use of standards is necessary but not sufficient for achieving the desired effects of e-Prescribing. Bell and colleagues evaluated two standards (Medication History Standard and Formularies and Benefits Standards) from the U. Apart from these two articles, four 45,632,663,799 other articles reported the use of commercial proprietary systems with medication management health feature sets. All the studies addressing the decision to use were based primarily on one or more of the feature sets discussed above (Table 26). Their important features were e-Prescribing, drug-drug interactions, calculation of dosing, and access to additional information. Six studies were on e-Prescribing with one being integrated with another 632 system and hand-held access. Some of the more important features addressed by these studies were e-Prescribing, medication lists, drug interaction and allergy alerts, receiving laboratory results electronically, changing doses, formularies, and order communication of prescription to 801 pharmacies. According to the study by Bell and colleagues, implementation of medication history standard and formulary and benefit standards in e-Prescribing would likely enhance usability of such systems if standard implementation was improved. Participants were dissatisfied with the unreliability of transmitting prescriptions successfully to the pharmacy, creating medication lists, recording of allergy information, and quantity of irrelevant and inappropriate alerts. Despite their complaints about alerts, participants preferred to continue receiving alerts as a safeguard against missing a major interaction. The important features were electronic connectivity for laboratory test results and orders, nursing and physician orders for medications, and prescription refills. Collectively, the important features were allergy checking, drug interactions, medication history, dosing calculation, medication formulation, and availability of laboratory test results. Data were collected from vendors by telephone interview and at sites where the systems were functioning, through direct observation of the systems and through personal interviews with prescribers and technical staff. Among the 60 e-Prescribing recommendations by Bell and 80 798 colleagues, 6 nine recommendations were not implemented by any of the ten systems. These included recommendations that would require e-Prescribing systems to handle prescription fulfillment data (their recommendations 10, 47, and 48), to use more complex drug benefit data (recommendation 22), and to use more advanced drug knowledge bases (recommendations 26 798,806 and 49). On average, the systems fully implemented 50 percent of the recommended 87 capabilities, with individual systems ranging from 26 percent to 64 percent implementation. Only 15 percent of the recommended capabilities were not implemented by any system. Intuitively, a system’s sustainability refers to its capacity to continue providing value. We believe that the most relevant available definition 9 comes from Humphreys and colleagues, who defined sustainability as the ability of a health service to provide ongoing access to appropriate quality care in a cost effective and health- effective manner. Our literature reviews revealed three important findings: although sustainability is mentioned frequently in the core informatics literature, it is poorly and infrequently defined, and none of the articles identified in the primary literature searching done to produce this evidence report explicitly studied sustainability. The legislation ties payments specifically to the achievement of advances in health care processes and outcomes. National Coordinator for Health Information Technology at the Department of Health and Human Services, “[this legislation] will lead us toward improvements and sustainability of our health care system that can only be attained with 809 the help of a reliable and secure nationwide electronic health information system. Overall, these features should help clinicians make better medical decisions and potentially avoid preventable errors. Future research should develop an operational definition of sustainability that can 89 be used to study its determinants. Summary overview of meaningful use objectives Source: New England Journal of Medicine, 2010. To what extent does the evidence demonstrate that health care settings (inpatient, ambulatory, long-term care, etc. Implementation Reports of implementation tend to be opinion pieces or descriptive studies. A number of articles looked at some or all of implementation, adoption rates, and factors related to adoption. The general findings for hospitals show that implementation and adoption are generally greater in larger, academic, urban, public hospitals. Adoption in primary care practices tends to increase with younger, recent medical grads, larger practice size, and also with more specialized physicians. They categorized barriers into physician and organizational resistance, cost and lack of capital, and vendor or product immaturity. This would include the workflows, culture, social interactions, and technologies in 822 place.
Lobectomy is considered the operation of choice buy discount biaxin 250mg gastritis back pain, but a pneumonectomy may be required to obtain negative margins 500 mg biaxin mastercard gastritis diet questions. Wedge resection has a higher incidence of local recurrence and is not recom- mended unless the patient cannot tolerate a lobectomy purchase cheapest biaxin and biaxin can gastritis symptoms come go. Patients who are not considered surgical candidates because of extensive disease or general medical condition are treated with chemotherapy and/or radiation. Preoperative Pulmonary Evaluation An assessment should be made to determine whether the patient can tolerate surgery. Evaluation of pulmonary function prior to surgery for non–small-cell carcinoma of the lung. Arterial blood gases should be drawn to assess for arterial hypoxia and hypercapnia. Patients who are short of breath at rest or upon minimal activity are considered poor surgical candidates. Studies currently are evaluating which patients with mediastinal (N2) lymph node metastasis will benefit from surgical resection. The 1-year survival for these patients is 20% to 37% and 5-year survival is 1% to 7%. Anderson trial ran- domized 60 patients to preoperative and postoperative chemotherapy and surgery versus surgery alone. The 3-year survival was 56% in the neoadjuvant group compared to 15% in the control group. The Spanish trial randomized 60 patients to preoperative chemotherapy followed by surgery and postoperative radiation, or surgery followed by radia- tion. This study also demonstrated a significant improvement in survival in the chemotherapy-treated group. With the addition of postoperative chemotherapy, 5-year survival rates up to 80% have been reported in patients with T1, N0, M0 disease. However, at present, surgery is not recommended even in patients with very limited disease. Surveillance Following Surgical Resection There has been no proven benefit to routine chest radiographs follow- ing a surgical resection of lung cancer. However, patients frequently are followed with chest radiographs every 4 months for the first 2 years, followed by chest radiographs every 6 months. A randomized trial comparing preoperative chemotherapy plus surgery with surgery alone in patients with non-small cell lung cancer. Langenfeld Summary When evaluating patients with hemoptysis, it is important to deter- mine whether the bleeding is massive and if the airway is secure. The treatment options used to control bleeding originating from the lung include medical management, bronchial lavage, embolization of bronchial arteries, and surgery. Critical in treating patients with lung cancer is determining the clin- ical stage. More advanced lung cancer is treated with chemotherapy with or without radiotherapy. Basic guidelines for the evaluation, staging, and treatment of lung cancer are highlighted (see Algorithm 13. Long-term results of lung metastasectomy: prognostic analyses based on 5,206 cases. Bronchial artery embolization for hemoptysis due to begin immediate and long-term results. Immediate and long-term results of bronchial artery embolization and life threatening hemoptysis. A randomized trial comparing pre- operative chemotherapy plus surgery with surgery alone in patients with non-small cell lung cancer. Induction chemoradiation and surgical resection for non-small cell lung carcinomas of the superior sulcus: initial results of S. To understand the difference between palliative and corrective surgery for congenital heart disease. The mother says she thinks he is short of breath at times and does not eat as well as his older brother did at the same age. Introduction The identification of a heart murmur early in life may be indicative of a significant congenital malformation of the heart. It is important to be able to differentiate potentially life-threatening lesions from benign processes. To do this, a basic understanding of these potentially complex lesions is necessary. When the diagnosis of a significant heart murmur seriously is considered, these infants must be referred to a pediatric cardiologist and pediatric cardiac surgeon for appro- priate diagnosis and corrective or palliative procedures. A relatively simple way to classify these potentially confusing lesions is according to categories based on the major presenting symptom: con- gestive heart failure or cyanosis (Table 14. Diagnosis of these lesions frequently can be made on the basis of the history and physical examination as well as with some basic noninterventional testing, 257 258 A. Cardiac catheterization in the diagnosis of these patients is required in fewer than 20% of all cases. Infants and children with congestive heart failure are symptomatic for either of two reasons: obstructing lesions or overcirculation of the lungs. Obstructive lesions leading to signs and symptoms of congestive heart failure involve the heart valves or the aorta. These include aortic stenosis, mitral stenosis, and various degrees of narrowing of the tho- racic aorta between the aortic valve and the level of the ductus arte- riosus. Initial presentation can range from a benign sounding heart murmur to life-threatening congestive heart failure. The symptoms caused by the obstructive lesion are attributed to blood backing up into the pulmonary circulation, causing pulmonary edema or congestion. Congestive heart failure also can be caused by left to right shunting of arterial blood, leading to overcirculation of the lungs. Abnormal communication can exist at the level of the atria (atrial septal defect), ventricles (ventricular septal defect), or in an extracardiac location (aortopulmonary window or patent ductus arteriosus signs). The most common symptoms that occur in this setting include recurrent upper respiratory infection, tachypnea, tachycardia, and failure to thrive. Oxygenated blood flows from the left side to the right side of the circulation because of the lower resistance and pressures in the right side of the heart. Excessive flow of blood through the pulmonary vasculature results in congestive heart failure and pulmonary hypertension. Pulmonary vascular resistance gradually increases due to this overcirculation from a complex interaction of factors. Even before Eisenmenger’s syndrome occurs, a high fixed resistance may preclude surgical correction. The infant in the case presented above is consistent with an infant who has either an obstructive lesion or a shunting lesion.