
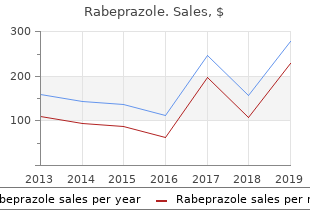
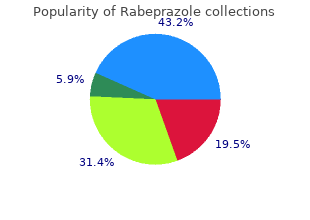
Adrian College. W. Pyran, MD: "Purchase Rabeprazole - Safe online Rabeprazole".
In this respect best buy for rabeprazole gastritis japanese, the presence of lung disease sufficiently severe to require postoperative ventilatory support is a relative contraindication to tracheal resection or reconstruction 10mg rabeprazole free shipping gastritis diet oatmeal. Monitoring of these patients should include placement of an arterial cannula in the left radial artery to permit continuous measurement of blood pressure during periods of innominate artery compression order rabeprazole 20mg with visa gastritis kefir. Numerous methods have been reported to provide oxygenation and ventilation of the lungs during these procedures. A small-bore anode tube may be placed through and distal to an upper tracheal lesion so resection may occur around the tube. Alternatively, an endotracheal tube may be passed through the glottis to above the stenosis, and a sterile endotracheal or bronchial tube may later be inserted into the trachea opened distal to the site of stenosis, with the sterile anesthesia tubing being led across the surgical field. After resection of the lesion, the sterile and distally placed endotracheal tube is withdrawn, and the 2636 upper tube (originally passed through the glottis) is advanced across the anastomosis. During these procedures, the patient is kept in a head-down position to minimize aspiration of blood and debris into the alveoli, and ventilation must be carefully monitored throughout the procedure. Clearly, the presence of a large-bore tube in the airway may make these resections technically difficult, and the use of high-frequency ventilation techniques may improve surgical access. Potential disadvantages of these high-frequency ventilation techniques are that, by necessity, the system is “open” (see “High-frequency Ventilation”), and egress of gas during exhalation may be compromised if the stenosis is tight. Also, the catheter may become occluded by blood and become displaced, and distal aspiration of debris or blood may occur. With complex resections, two anesthesia teams with two machines and anesthesia circuits or sets of ventilating equipment may be necessary to ensure adequate ventilation of the two distal airway segments. After tracheal resection or reconstructive surgery, patients should be kept with the neck and head flexed to reduce tension on the anastomotic suture lines. In some cases, this is maintained by using sutures between the chin and the anterior chest wall. Extubation of the trachea is performed as early as possible to minimize tracheal trauma due to the endotracheal tube and cuff. Bronchopulmonary Lavage This procedure involves irrigation of the lung and bronchial tree, and is used as a treatment for alveolar proteinosis, radioactive dust inhalation, cystic fibrosis, bronchiectasis, and asthmatic bronchitis. If involvement is equal, the left lung is generally lavaged first because gas exchange should be better through the larger, right lung. Patients are premedicated and supplied with supplemental oxygen en route to the operating room. Monitoring should include an arterial catheter, and a stethoscope should be placed over the ventilated lung to check for rales, the presence of which may indicate leakage of lavage fluid into this lung. Before lavage, this serves to denitrogenate the lungs so only oxygen and carbon dioxide remain. Instillation of fluid then allows these gases to be absorbed, resulting in greater access by the fluid to the alveolar spaces than if the more insoluble nitrogen bubbles remained. With the patient in a head-up position, warmed heparinized isotonic saline is infused by gravity from a reservoir 30 cm above the midaxillary line into the catheter to the dependent lung, while the nondependent lung is ventilated. When fluid ceases to flow in (usually after 700 to 1,000 mL in an adult), the patient is placed in a head-down position and fluid is allowed to drain out. The lavage is continued until the effluent is clear (as opposed to the milky fluid that drains initially when lavage is being performed for alveolar proteinosis), at which point the lung is suctioned and ventilation is re- established with large V (and pressures) because compliance is decreasedT owing to loss of surfactant. With each lavage, inflow and outflow volumes are monitored so the patient is not “drowned” in fluid, and there is no excessive absorption or leakage to the ventilated side. Two-lung ventilation is re-established and, as compliance improves, an air–oxygen mixture (addition of nitrogen) may be introduced to help maintain alveolar patency. After a further period of ventilation, in most patients, the trachea can be extubated in the operating room. In the posttreatment period, patients are encouraged to cough and engage in breathing exercises to fully re-expand the treated lung. From 3 days to 1 week after lavage of the first lung, the patient may return to the operating room for lavage of the other lung. Problems sometimes encountered with this procedure include spillage of lavage fluid from the treated to the ventilated lung. This must be managed by stopping the lavage and ensuring functional separation of the lungs before continuing. During periods when lavage fluid is being instilled into the dependent lung, oxygenation usually improves because the increased intra-alveolar 2638 pressure caused by the fluid produces diversion of the pulmonary blood flow to the nondependent, ventilated lung. Conversely, when the fluid is drained out of the dependent lung, hypoxemia may occur. In some cases in which severe hypoxemia was anticipated during right lung lavage, the risk has been reduced by passing a balloon-tipped catheter into the right main pulmonary artery (checked by radiography) and inflating the balloon during periods of right lung drainage. In this way, blood flow to the dependent, right, nonventilated lung is minimized during periods of drainage. In such cases, cardiopulmonary bypass may be required to provide oxygenation during lavage. The incidence in children and adolescents aged 0 to 19 years was found to be between 1 and 5/1,000,000 per year. These rates may well be an underestimate of the true incidence rates, as mild cases will have been missed and cases in the elderly will have been misdiagnosed. In some cases, the disease is generalized and may involve the bulbar musculature, causing problems with breathing and swallowing. Peripheral muscle involvement may cause weakness, clumsiness, and difficulty in holding up the head or in walking. Studies of the endplate area show loss of synaptic folds and a widening of the synaptic cleft. The electrical counterpart of this is a decrement in the compound muscle action potentials evoked by repetitive stimulation of a motor nerve. Mechanical and electrical (electromyography) decrements improve with 2 to 10 mg of intravenous edrophonium (Tensilon test). When the routine electromyographic results are equivocal, a regional nondepolarizing muscle relaxant test may be performed using a tourniquet to isolate the limb and limit the action of the drug. In the regional nondepolarizer muscle relaxant test, electromyograms are performed before and after the administration of 0. Overdosage causes the muscarinic effects of acetylcholine and may cause a cholinergic crisis. In a patient with weakness, distinction between the two types of crisis may be made by performing a Tensilon test or by examining pupillary size, which will be large (mydriatic) in a myasthenic crisis but small (miotic) in a cholinergic crisis. Steroids are used for short-term immunosuppression, whereas for long-term effect azathioprine, cyclophosphamide, cyclosporine, methotrexate, mycophenolate mofetil, rituximab, and tacrolimus have been used. Rapid short-term immunomodulation has been 2641 achieved in acute exacerbations or to improve muscle strength prior to surgery. Plasmapheresis causes a decrease in plasma cholinesterase levels that may prolong the effect of drugs such as succinylcholine that are normally broken down by this enzyme system. After thymectomy, approximately 75% of patients either go into remission or show some improvement.
Cumin des Pres (Caraway). Rabeprazole.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96237
Diseases
A trocar is used the most convenient position purchase rabeprazole discount gastritis diet 91352, and a bicortical screw is placed (a to achieve perpendicular screw placement rabeprazole 10 mg on-line gastritis tums. Next rabeprazole 10 mg discount gastritis symptom of celiac disease, the plate with a monocortical screw may be placed if the location is close to the screw in the most anterior-superior hole is positioned, and the inferior alveolar nerve canal). All other screw holes are drilled, screw is engaged with a screwdriver and partially tightened. Before the vertical cut is complete, a nine-hole, maxilla, a maxillary vestibular incision is made and the zygomati- curved plate is placed from the coronoid process above the hori- comaxillary buttress is exposed bilaterally (Figure 32-3, A). Unless contraindicated, a preoperative A number of intraoperative complications are possible. If the horizontal osteotomy is 24 hours) can be used, in addition to a universal pressure head extended too far posteriorly, there is the risk of fracturing wrap, to prevent swelling and hematoma. Tis sequela can be prevented by thorough control of nal fxation much more challenging. Most often, postoperative bleeding is related to the short in the anteroposterior dimension, the vertical oste- retromandibular vein. However, profuse arterial bleeding is otomy that connects with the posterior aspect of this possible and may require external carotid artery ligation or 11 osteotomy is likely to injure the inferior alveolar neuro- embolization. Tis is especially true with the extra- Postoperative nausea and vomiting (N/V) and dehydra- oral approach because there are no good guidelines to tion can occur for many reasons. Some triggers of N/V indicate where the inferior alveolar nerve is in relation to include anesthetic agents, pain, narcotic analgesics, and 12-14 the lateral surface of the mandible. With the extraoral approach, there is is an important tool in the management of this 11 a risk of injury to the marginal mandibular branch of the complication. Te prevention of infections after usually results from transection of the inferior alveolar, orthognathic surgery is afected by factors such as the patient’s masseteric, or maxillary artery. If bleeding occurs, it usually age and immune status and the surgeon’s experience (which can be controlled with tamponade (packing). Routine use of perioperative intravenous antibiotics for 24 hours and postoperative antibiotics should minimize this complication. Postoperative Considerations Some postoperative complications include excessive swelling, hemorrhage or hematoma, postoperative nausea and vomit- ing, infection, mandibular dysfunction, and relapse. Kobayashi A, Yoshimasu H, Kobayashi J, the statistical relationship between the true inverted L osteotomy: report of three cases, Amagasa T: Neurosensory alteration in the lingula and the antilingula, Int J Oral Maxil- J Oral Maxillofac Surg 67:435, 2009. Van Sickels Armamentarium #9 Molt periosteal elevators (two) Fissure burs (if third molars are present) Needle electrocautery A series of chisels and one curved chisel Hargis retractor Pear-shaped bur or round bur (if Appropriate sutures J-strippers mandible is to be set back) Bipolar electrocautery (if necessary) Jeter–Van Sickels bone clamp Reciprocating saw Coronoid notch retractor Kelly hemostat Wire pushing instrument (“pickle Curved Kocher clamp with umbilical Local anesthetic with vasoconstrictor fork”) tape Minnesota retractor History of the Procedure correct asymmetry. Although there have been many modifcations designed to Others have shown that although closing an open bite 13,14 improve the procedure, two of the earlier ones were suggested reduces stability, in selected instances it can be used. It 4 design is Epker, who in 1977 published a paper showing is clear that taking out the third molars at the time of the several modifcations and emphasizing the need to maintain sagittal split takes a little longer and also that many factors the blood supply to the proximal segment. Since his publication in 1988, many alternatives have been used in the application of screws and/or plates to fx the segments. Today the bilateral sagittal split, in its multiple iterations, is the most commonly used osteotomy for As noted previously, there are several areas of controversy moving the mandible. Tese the length and design of the osteotomy on the proximal include its use to close an open bite and whether third molars segment and the type of fxation used. Tere is a higher incidence of inferior alveolar nerve injury with a bilateral sagittal split osteotomy than with a vertical Indications for the Use of the Procedure ramus osteotomy when used to set back the mandible. However, a bilateral sagittal split can be more consis- Te bilateral sagittal split is an extremely versatile procedure tently fxed with plates and screws and hence allows the that can be used to advance the mandible, set it back, or patient earlier function. Te more the mandible is set back, the more it tends lengthen the mandible gradually. Tis instability For large advancements that can be achieved with a sagit- or relapse may be due numerous factors. Tese include extending the Dal Pont general, if a large setback is required to achieve an ideal modifcation a little farther forward and using more rigid occlusal result, a component of maxillary hypoplasia usually forms of stabilization for the osteotomy. As such, the patient would have a more stable and maxillary fxation with skeletal stabilization in the form of better esthetic result with two-jaw surgery. Place a curved Kocher clamp with umbilical tape Elevate the mucosa and connective tissue enough to expose the tied to it at the tip of the coronoid and secure it to the drape. Elevate the tissue along the medical aspect of the mandible to Release the tissues in a subperiosteal plan to the tip of the expose the lingual fossa (Figure 33-1, B). Continued A B Figure 33-1 A, Just before incision, the Minnesota retractor is in place, and the incision has been outlined. B, Kocher clamp is in place; periosteal elevator is on the medical aspect of the mandible just distal to the neurovascular bundle. This bone Use a reciprocal saw at a 45-degree bevel to cut the bone from cut is usually stopped at the distal aspect of the second molar the lingual fossa to the anterior ramus. The surgeon must make sure the bone cut is complete and is removed, and the lateral soft tissues are dissected. Depending is beveled at approximately a 45-degree angle at the inferior on the amount of advancement needed, the lateral bone cut is border (Figure 33-1, D). Gentle prying of the bone should result in symmetric elevator is used to retract the lingual tissue on the medical aspect expansion of the osteotomy. A spatula chisel or small beveled chisel is used used to spread the segments; the author’s preferred technique is to check the medial bone cut, and the split is begun with gentle to use a series of chisels to slowly pry the segments apart. Fre- progressive tapping of the chisel along the entire distance of quently, a small curved chisel is used at the inferior border of the the ascending ramus. Progressive spreading of the segments is mandible to initiate the inferior split of the mandible, ensuring achieved with this maneuver. If the segments do not spread that it propagates along the inferior border (Figure 33-1, E). C D E1 E2 Figure 33-1, cont’d C, Saw cut beveled on the medial aspect, extending down the ascending ramus just short of the second molar. D, Lateral cut at a 45-degree angle at the inferior border, extending upward approximately at the mesial aspect of the second molar. Before placement of the clamp, any interference that into its preplanned position and the patient is placed in maxillo- prevents the segments from lying passively against one another mandibular fxation. A “pickle fork” is used to frmly set the proximal ments posterior into the glenoid fossa and to align the inferior segment, and the inferior borders usually are aligned before place- border of the proximal segment with the distal segment. For larger advancements a more rigid plate is bicortical screws are placed, usually via a transcutaneous used. Once both sides have been temporarily fxed, the maxillo- approach (Figure 33-1, G). On the left is a more rigid plate; on the right, a less rigid adjustable plate was used. A Jeter–Van Once the mandible has been placed into occlusion, the overlap Sickels bone clamp is used again to achieve temporary fxation. A portion of The ascending ramus of the proximal segment often must be the proximal segment is removed so that the segments ft together.