
Institute for Christian Works. P. Bandaro, MD: "Order Sarafem online - Discount online Sarafem no RX".
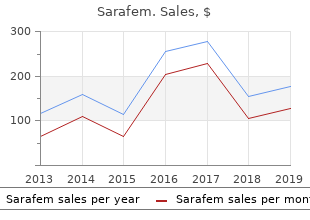
It is important to pursue these findings as they could indicate barriers to quality and timely care buy 20 mg sarafem with mastercard breast cancer, potentially amenable to intervention and prevention order sarafem 10mg otc menstruation every 20 days. A further element of complexity is the presence of trends and factors that will likely change the landscape of congenital heart defect buy sarafem 20mg with visa menstruation 9 tage, though at different rates across countries and healthcare systems. A few such trends are worth discussing, as they could have a significant impact on the lives of people and on communities. It may be more helpful to briefly surmise some forces that will likely drive these changes, as these forces will vary in different places and times. Changes in the total prevalence of congenital heart defects (the sum of live births, stillbirths, and pregnancy terminations) will depend on the balance of risk factors and protective factors in a population. Diabetes, several chronic illnesses, and obesity are affecting more (and sometimes younger) people in many developed and developing countries. Also, demographic trends suggest an increasing maternal age at conception in many developed countries. This shift would lead to more pregnancies at higher risk of maternal-age dependent chromosomal syndromes (e. The increase would likely be small on a yearly basis, and probably undetectable unless the data are examined carefully. The prevalence at birth of these heart defects would also depend on the concurrent use of fetal diagnosis and pregnancy termination. As a risk factor, the population distribution of maternal age is difficult to modify, though education and preconceptional counseling could have an impact in individual situations. Yet, some factors offer hope: there appears to be now greater attention to integrated preconception health, and, in the areas of P. Whether these initiatives will reverse the current worrying trends remains to be seen. Prenatal diagnosis will likely have a significant impact on occurrence and outcomes, though its direction and magnitude are not entirely predictable. In some areas, pregnancy terminations account for a substantial fraction of cases of selected congenital heart defects. In a study from Europe with data through 2005, 6% of all cases of heart defects not associated with chromosomal anomalies were terminations of pregnancy, with variations across registries and type of congenital heart defect (13). Notably, the reported rate of prenatal diagnosis was fairly low (13%) suggesting that as prenatal detection rates increase, terminations of pregnancy could account for a higher fraction of cases in the future. In the latest annual report (2012) from the International Clearinghouse for Birth Defects Surveillance and Research (Fig. Clearly, failure to incorporate pregnancy terminations will underestimate the overall occurrence and impact of congenital heart defects. Failure to consider pregnancy terminations can also bias etiologic studies, for example, if an exposure (e. Diagnosis is typically easier than treatment; in countries with increasing medical technology, such as large parts of Asia and Africa, rates of prenatal diagnosis of severe heart defects will likely increase, at least initially without corresponding availability of effective and affordable treatment: depending on the social context, pregnancy terminations due to fetal anomalies could increase. Conversely, with better treatment options, family choices may change and birth prevalence of some severe heart defects could even increase, if cases previously terminated prenatally are allowed to reach birth. Prenatal diagnosis could also decrease morbidity and mortality if it decreases delayed diagnoses and promotes better organization of care. Newborn screening for critical congenital heart defects using pulse oximetry is being implemented in several areas with the goal of detecting at birth certain critical congenital heart defects (115,116,117,118,119). Appropriately implemented, newborn screening should increase early diagnoses of some severe heart defects: the rationale is that outcomes should then improve, because treatment would start promptly (before closure of the ductus arteriosus) and in a well-prepared healthcare setting. From the perspective of outcome evaluation and birth prevalence, universal screening could promote the rapid and complete identification of the heart defects with greatest public health impact. While high-quality registries with multiple sources of ascertainment and extended followup would be unlikely to miss many such cases, the linkage between neonatal screening and epidemiologic surveillance could lead to significant improvements in data quality in the many areas with only basic registries or none at all. Appropriately leveraged, universal screening would create a valuable repository of information on selected major congenital heart defects for the entire screened population. Such population- based data would provide a powerful basis not only for monitoring prevalence, but also in assessing outcomes, conducting etiologic studies, and evaluating prevention interventions. As more babies survive longer, their use of healthcare resources will likely increase. In general, congenital heart defects are likely to remain one of the more costly birth defects—by way of comparison, most children with orofacial clefts can be effectively “cured” by early surgery and lead an essentially normal and productive life, unlike many children with complex heart defects who will require long-term treatment and repeat surgeries. However, earlier diagnosis, through prenatal or newborn screening, could theoretically decrease costs if it substantially reduces preoperative morbidity and postoperative complications; to date, these benefits remain unproven. Deaths due to congenital heart defects (as for birth defects in general) will likely increase as a proportion of infant deaths, as infant deaths due to other causes (infections, prematurity) decline. In absolute terms, however, mortality should decrease gradually with better treatment and earlier diagnoses. Lower mortality will translate in greater longevity: prevalence in adults will increase, with greater needs for specialized care. Unless adequate services for older individuals are provided, the peak of mortality for heart defects risks being delayed rather than decreased. Finally, some factors may lead to an apparent change in mortality unrelated to true improvements in outcomes. For example, increased pregnancy terminations for fetal cardiac defects can cause an apparent reduction in mortality as a proportion of the population (as it is usually tracked using death certificate data), because fewer babies will be born with heart defects and would be at risk for dying. Including pregnancy terminations in birth defect surveillance would help avoid this bias. Conversely, as screening and diagnostic technology is introduced in a country in which it had not been available previously, deaths P. A different concern is the unexpected, unpredictable introduction in a population or region of a teratogen—for example, retinoic acid—causing a cluster of congenital heart defects. Early detection of such teratogen-induced “epidemics” of birth defects is a stated goal of many monitoring programs. Medications and environmental exposures are particular concerns for the general public and the ability to respond to these concerns quickly and in a cost-efficient manner is a significant benefit of having a high-quality monitoring system in place. Effective monitoring must balance the ability to detect true changes (high sensitivity, low false-negative rates) with the cost of investigating false alarms (false-positives). This requires a system that is able to select, among the continuous stream of monitoring signals, those with the greatest epidemiologic and biologic plausibility. Epidemics can be missed by setting the bar too high (the signal is not picked up) or too low (because limited resources are spread across too many futile investigations). Practical challenges include the presence of local or global trends that can shift background rates, missing cases by not ascertaining pregnancy terminations, and low-quality data when diagnosis is based on administrative data sets (e. Rising to these challenges requires increased resources and innovative approaches, some of which are summarized in Table 2.
It is a surprising fact that a wedge- or lens-shaped opacity may be very diffcult to see because of the way it fades out at its margins buy sarafem 10 mg on-line pregnancy 26 weeks, but if such a lesion is in contact with the mediastinum or diaphragm these will lose their normally sharp outlines purchase sarafem 20mg otc breast cancer 10 year survival rate. Radiological signs of lung disease It is helpful to try and place any abnormal intrapulmonary opacities into one or more of the broad categories shown in Box 2 purchase sarafem 20 mg visa women's health problems and solutions. Air-space opacifcation means the replacement of air in the alveoli by fuid or other materials (e. The fuid can be either an exudate (often called ‘consolidation’) bronchi contrasts with the fuid in the adjacent lung. The signs of consolidation are: • The silhouette sign, namely loss of visualization of the • An opacity with ill-defned borders (Fig. Consolidation of a whole lobe, or the majority of a lobe, is • An air bronchogram (Fig. The diagnosis sible to identify air in bronchi within normally aerated of lobar consolidation requires an appreciation of the radio- lung, because the walls of the normal bronchi are too thin logical anatomy of the lobes (see Fig. However, if the alveoli are flled with fuid, the air in the Because of the silhouette sign, the boundary between the affected lung and the adjacent heart, mediastinum and dia- phragm is invisible. The air is then seen as a transradiancy within the consolidation and an air–fuid level may be present (Fig. Pulmonary collapse (atelectasis) The arrow points to a bronchus that is particularly well seen. Collapse caused by bronchial obstruction Cavitation (abscess formation) within consolidated areas in the lung may occur with many bacterial and fungal Collapse caused by bronchial obstruction occurs because infections (Fig. Abscess formation is only recogniza- air cannot get into the lung in suffcient quantities to replace ble once there is communication with the bronchial tree, the air absorbed from the alveoli. The signs of lobar col- allowing the liquid centre of the abscess to be coughed up lapse are: (a) (b) Fig. The heart border and the medial half of the right hemidiaphragm are visible, whereas the lateral half is invisible. Fluid levels are only visible if the chest radiograph is taken with a horizontal x-ray beam. The presence of air or fuid in the pleural cavity allows the The commoner causes of lobar collapse are: lung to collapse. In pneumothorax, the diagnosis is obvious • Bronchial wall lesions, usually primary carcinoma, but but if there is a large pleural effusion with underlying pul- occasionally other bronchial tumours such as carcinoid monary collapse it may be diffcult to diagnose the pres- tumours. The mediastinum and diaphragm may move towards the Linear atelectasis collapsed lobe. The result Chest 35 Trachea deviated to right Position of Horizontal oblique fissure fissure pulled down Oblique fissure Dense shadow due to pulled down overlapping of opaque (a) (b) right lower lobe on heart Fig. Chest 37 Horizontal fissure Trachea deviated Oblique fissure pulled up to right pulled up Horizontal fissure pulled up (a) (b) Fig. The upper two-thirds of the left mediastinal and heart borders are invisible, but the aortic knuckle and descending aorta are identifable. The visible portions of the aorta have been Oblique fissure drawn in for greater clarity. On the lateral view, the upper lobe pulled upward can be seen collapsed anteriorly. Note the smooth lateral border of the collapsed lobe formed by the displaced oblique (major) fssure (arrow). The scan shows compensatory overexpansion of the left upper lobe, which has crossed the midline anterior to the aortic arch (A). Metastasis is very unlikely in a patient without a known extrathoracic primary malignant tumour, but is an important considera- tion in those who are known to have such a tumour. Hamartomas and granulomas are best left alone, whereas bronchial carcinoma, active tuber- culosis and lung abscess require specifc treatment. Assessing the rate of growth of a spherical lesion in the The collapsed lobe (arrows) can be clearly seen beneath the large lung is one of the most important factors in determining left pleural effusion. Failure to grow over a period of 18 months or more is a strong pointer to either a benign tumour or an inactive granuloma. An is a horizontally orientated band or disc of collapse (see enlarging mass is highly likely to be a bronchial carcinoma Fig. Spherical opacities (lung mass, lung nodule) Calcifcation The diagnosis of a solitary spherical opacity in the lung The presence of calcifcation is the other vital observation, (solitary pulmonary nodule) (Fig. Calcifcation is a common When a nodule is discovered in a patient who is over 50 fnding in hamartomas, tuberculomas and fungal granulo- and a smoker, bronchial carcinoma becomes the major con- mas. The patient’s symptoms may be is of great value in detecting calcifcation in a solitary pul- monary nodule. Tumours of the lung apex are par- • Metastasis ticularly liable to invade the chest wall and adjacent bones • Lung abscess (Pancoast’s tumour). The central focculant (‘popcorn’) calcifcation is typical of that seen in hamartomas. Shape of the opacity Primary carcinomas are nearly always rounded with a lobulated, notched or infltrating outline (Figs 2. Even if only one small portion of a round lesion has an irregular or lobular edge, the diagnosis of primary car- cinoma should be seriously considered. The rest of the flm should be checked carefully after a single lung mass has been found. It does not occur in is primarily to characterize the nodule using the following benign tumours or inactive tuberculomas. As mentioned above, extensive calcifcation of a inner or outer walls are irregular, the diagnosis of carci- nodule effectively excludes primary carcinoma of the lung noma is highly likely. Lung abscesses of this or percutaneous needle biopsy in cases where the position size, however, virtually always show cavitation and round of the nodule is diffcult to defne on conventional flms. Only Occasionally, this pattern is seen with abscesses, other neo- a small proportion, notably very small tumours (<1 cm) and plasms or with granulomas caused by fungal infection, slow-growing cancers, do not show increased uptake. Septal lines The interlobular septa within the lung are connective tissue Role of needle biopsy planes containing lymph vessels. They are normally invis- Transthoracic needle biopsy, using either fne needle aspi- ible. Unlike malignant neoplasm, so the technique should only be used the blood vessels they often reach the edge of the lung. The septal lines (arrow) are seen in the outer centimetre of lung where blood vessels are invisible or very diffcult to Fig. There are two important causes of thickened interlobular septa: The pleural edge in a pneumothorax is seen as a line • interstitial pulmonary oedema approximately parallel with the chest wall. Pleuropulmonary scars and linear (discoid) atelectasis Widespread small pulmonary opacities These two conditions are common causes of line or band- like opacities and are somewhat similar in appearance.
J Thorac nates: experimental study with neonatal rabbits from birth to Cardiovasc Surg 1995 buy discount sarafem on-line women's health center upper east side;110(4 Pt 2):1255–64 buy sarafem 20 mg on line women's health clinic nelson. Organ preserva- cardioplegia on high energy phosphate kinetics during cir- tion solutions in heart transplantation – patterns of usage and culatory arrest with deep hypothermia in the newborn piglet related survival sarafem 20 mg low cost menopause gifts. Single-dose versus multidose car- dioplegia solutions using thermodilution cardiac output in dioplegia in neonatal hearts. Detrimental effects of crystalloid cardioplegia for repair of ventricular septal defects multidose hypothermic cardioplegia in the neonatal heart: in pediatric heart surgery: a randomized controlled trial. Ann versus multidose blood cardioplegia in arterial switch proce- Thorac Surg 2005;80:989–94. Ann temperature correlates with increased white cell activation Thorac Surg 2006;82:172–8. J Thorac sary adjunct to cardioplegic protection and cause of pulmo- Cardiovasc Surg 1992;103:219–29. Rapid cooling between calcium and magnesium in pediatric myocardial pro- contracture of the myocardium. Warm induc- induction of cardioplegia with glutamate-enriched blood in tion blood cardioplegia in the infant. J Thorac Cardiovasc coronary patients with cardiogenic shock who are dependent Surg 1990;100:896–901. Dexamethasone ervation in neonatal lambs: comparison of hypothermia with pretreatment provides antiinfammatory and myocardial pro- crystalloid and blood cardioplegia. Pediatric Cardiology, 6th comes associated with intraoperative steroid use in high-risk ed. The effect of tepid amino acid-enriched induction cardioplegia on the outcome of infants undergoing cardiac surgery. However, his frst patient, a The pathophysiology of congenital heart disease is limited to 15-month-old baby had died and the subsequent two chil- three main problems. There may be a volume load in which dren died leading Gibbon himself to abandon any further one or both ventricles must pump more than the usual amount open heart surgery. This is most commonly because of excessive pul- tiple deleterious effects that were particularly dangerous monary blood fow resulting from a septal defect. The priming volume for early circuits be a pressure load for one or both ventricles. This is usually was usually several liters, which necessitated exposure of an secondary to obstruction to outfow from the affected ventri- infant to what was effectively a massive blood transfusion of cle. The infammatory to reduced pulmonary blood fow but also may be because mediators, such as bradykinin and complement,2 that were of inadequate mixing between two parallel circulations as released in large quantities as part of the “systemic infam- in transposition of the great arteries. Early procedures were matory response” to bypass were particularly problematic designed to palliate but not cure these problems, thereby for the neonate and young infant who have a propensity to allowing the child to grow to an age and size at which “cura- greater vascular permeability and tissue edema than the tive” surgery was thought to carry a lesser risk. Robert SyStemic to Pulmonary arterial ShuntS Gross who had performed the frst repair of coarctation in the United States recommended deferring repair until at least 10 A systemic to pulmonary arterial shunt reduces cyanosis by years of age. Although this is a concep- Anesthesia for babies was in its infancy and intensive tually simple procedure, it nevertheless carries a number of care units appropriate for young babies did not exist in the important challenges for the surgeon. Diagnosis of heart disease was dependent on the inva- size of the shunt must be appropriate for the size of the child. Surgeons did not have microvascular of the child, what may be large enough for the child at the instrumentation or the knowledge of delicate surgical tech- time of the procedure may not be large enough in the future. For all these reasons, volume load on one or both ventricles so the child will have every attempt was made to manage the child medically and traded the problems of cyanosis for the secondary problems to defer surgery until the child was considered to be better associated with a volume load, most notably congestive heart able to withstand the stresses of surgery. Flow into the lungs could not be managed medically, a number of ingenious pal- during diastole lowers diastolic blood pressure and results in liative surgical procedures were developed. Blalock had discovered, perhaps without realizing it, that the size of the subclavian artery happened to be appropriate for supplying enough, but not too much, pulmonary blood fow. Furthermore, it had growth potential and could there- fore sustain the child for many years. However, in these early years which predated the development of vascular surgery and certainly predated microvascular surgery, the procedure was technically demanding for many surgeons, particularly working with small babies. Unless the anastomosis was con- structed perfectly, there was a high risk of shunt thrombosis. This led others to seek a technically simpler procedure with a higher probability of patency. Waterston Shunt The Waterston shunt is an anastomosis between the ascend- ing aorta and the right pulmonary artery. This oxygenator was used at St Vincent’s a left thoracotomy with a side-biting clamp applied to both Hospital, Melbourne, Australia in the mid-1970s. The Potts shunt has all the disadvantages of the Waterston shunt and in addition is very diffcult to take down. The modifed Blalock shunt was introduced by deLeval The Blalock–Taussig Shunt et al. Optimal Timing for Congenital Cardiac Surgery 221 between 3 and 6 mm in diameter is anastomosed to the left artery distortion. However, even a perfect Blalock shunt subclavian artery and the left pulmonary artery. The left sub- requires dissection of the right or left pulmonary artery, clavian artery is said to limit fow to an appropriate amount which is followed by adventitial scarring. Even if a stenosis and by using a larger graft the child is able to grow without cannot be seen it is very likely that the vessel wall compli- becoming excessively cyanosed. Modifcations of this shunt ance is decreased in the region of dissection and anastomo- are presently the most popular systemic to pulmonary artery sis. All of the palliative procedures result in some degree of shunt (see Chapter 25, Three-Stage Management of Single intrapericardial scarring which can obscure important car- Ventricle, for technical details). The high pressure and high fow in the Presence of Congenital Heart Disease pulmonary arteries will eventually lead after a year or two Because palliative procedures do not correct, but simply to irreversible damage to the pulmonary microcirculation, palliate congenital cardiac pathology, there will be ongoing that is, pulmonary vascular disease. For fed Blalock shunt, a band has the problem that it does not example, in the case of transposition physiology, not only is allow growth so that what may be an appropriate degree of there ongoing cyanosis, but in addition the most cyanosed band tightness for an infant will be too tight for the older blood is delivered to the coronary arteries and brain during child. Thus, the child will become increasingly cyanosed the period of critically important brain and heart develop- with growth. On the other hand, early monary artery that can lead to permanent distortion at the primary repair creates a physiologically normal circulation origins of the right and left pulmonary arteries and/or distor- which allows normal maturation of the individual. Infow occlusion with hypothermia was introduced ing of the parallel pulmonary and systemic circulations, the at the University of Minnesota in 1953,15 but suffered from the child will die from cyanosis. The procedure is performed through a of the advantages of early repair was provided by C Walton right thoracotomy. Incisions are made anterior and posterior to the low morbidity and mortality and excellent long-term results. With the advent of the Rashkind balloon septostomy nique fell into disrepute and attention was focused on open in 1966, it was rarely necessary to perform this procedure. Ladd New Zealand during the late 1960s that primary correction of Professor of Surgery at Harvard Medical School and Children’s congenital heart anomalies during infancy could be performed Hospital Boston. Castaneda, like Barratt-Boyes, popularized with a low mortality if exposure to cardiopulmonary bypass was the concept of primary repair of congenital heart disease during minimized. John Kirklin, a long-time and To fully appreciate the advantages for the heart of early very vocal opponent of early primary repair entitled his key- repair versus an approach of palliation, it is necessary to note address, “The movement of cardiac surgery to the very 21 have a thorough understanding of the transition that occurs young.
However cheap sarafem 10 mg overnight delivery breast cancer pumpkins, several other features are also important to understand the double helix cheap sarafem 10 mg otc breast cancer 6 cm. Given the constraints of the bond angles of the bases and sugar phosphates buy discount sarafem 20 mg women's health vernon nj, the double helix could not be constructed easily if both chains ran parallel to each another. One chain of the helix runs in the 5 to 3 orientation, and the other chain runs in the 3 to 5 orientation. The 5 and 3 nomenclature is derived from the numbering system of the sugar ring that we saw in Figure 1. Additional nucleotides are joined to the chain through phosphodiester bonds, which link the hydroxyl group on the 3 carbon atom of one sugar with the phosphate on the 5 carbon atom of an adjoining sugar. The chain terminates in a free hydroxyl group on the 3 carbon atom of the last sugar. The bases on one strand of the helix are complementary to those on the opposite strand, A always base pairs with T and G always base pairs with C 1. The arrangement is best illustrated by inspection of a computer- generated model of high-resolution crystal X-ray diffraction data (Figure 1. It can be noted that the base pairs are not all perpendicular to the helical axis, and that some show propeller twist, where the purine and pyrimidine pair do not lie flat but are twisted with respect to each other, like the blades of a propeller (Dickerson, 1983). The pairing of a purine (A or G) with a pyrimidine (T or C) within the helix is important for the integrity of the helix. Oxygen atoms are coloured red, phosphorus is orange, carbon is white and nitrogen is blue The constant length of the purine–pyrimidine pairing would be disrupted if purine–purine (too large) or pyrimidine–pyrimidine (too small) pairings occurred. The grooves along the helical axis do, however, provide a mechanism whereby the bases can be distinguished from one another. This is a result of the glycosidic bonds that attach a base pair to its sugar rings not lying directly opposite each other across the helical axis. As a result, the two sugar–phosphate backbones of the double helix are not equally spaced along the helical axis, and the grooves that form between the backbones are not of equal size. The floor of the major group is composed mainly of nitrogen and oxygen atoms that belong to the unique portions of each base pair. In contrast, the floor of the minor groove is filled with nitrogen and oxygen atoms that are generally common to either the purines or to the pyrimidines. Thus, the potential of the major groove for interactions shows a much greater dependence on base sequence than that of the minor groove. The α-helix, originally postulated by Pauling and Corey in 1951, is a protein secondary structure motif in which a right-handed helix is formed by amino acids on a polypeptide chain (Pauling et al. This raises several important questions – what is a hydrogen bond, and is it sufficiently strong to maintain the integrity of the double helix? To address the first question, a hydrogen bond is a weak electrostatic interaction between a covalently bonded hydrogen atom and an atom with (a) (b) 22 11 33 44 55 55 11 44 33 22 Figure 1. The hydrogen atom assumes a partial positive charge, while the unshared electron pair assumes a partial negative charge. In general terms, a chemical bond is an attractive force that holds atoms together. The spontaneous formation of a bond between two free atoms involves the release of internal energy of the unbonded atoms and its conversion to another energy form, e. The strength of a particular bond is measured by the amount of energy released upon the formation of the bond. The change in energy ( G)that accompanies bond formation is used to describe the strength of a bond. As found in the double helix, adenine forms two hydrogen bonds with thymine, and cytosine forms three hydrogen bonds with guanine (see Figure 1. For short regions of complementation, the equation above breaks down, and the following estimation (sometimes called the Wallace rule) is used to determine the Tm (Wallace et al. As the temperature falls, the thermal energy that was used to break the hydrogen bonds between the strands is reduced, and random collisions between the complementary strands will result in their re-association. Providing that the temperature is reduced ◦ relatively slowly (1–2 C per second), complete duplex formation will result. As we will see in Chapter 3, understanding how cells deal with these plasmids has played a pivotal role in advances in molecular biology and genetic engineering. A twist in the molecule will result in the formation of a positive (+)anda negative (−) supercoil. This number corresponds to the number of double- helical turns in the original linear molecule. The linking difference ( Lk)givesan indication of the overall levels of supercoiling within a molecule (Figure 1. An appropriate analogy here is to think about how you would unkink a twisted garden hosepipe. At the end, the rotation of the pipe itself will result in the release of the kink. Coming back to the hosepipe analogy, another way to remove the kinks (although less practical in the garden) would be to cut the pipe to create new ends near the site of the twist. The pipe could then be untwisted locally and resealed to remove the kink and reform the pipe. During interphase, the genetic material (together with its associated proteins) is relatively uncoiled and dispersed throughout the nucleus as chromatin. When mitosis begins, the chromatin condenses greatly, and during prophase it is compressed into recognizable chromosomes. The particles occur regularly along the axis of a chromatin strand and resemble beads on a string. These particles, initially referred to as ν-bodies (Olins and Olins, 1974), are now called nucleosomes. The high-resolution structure also revealed that the amino-terminal ends of some of the histones protrude from the octamer and project away from the nucleosome. The significance of the amino-terminal tails is that they have the potential to interact with adjacent nucleosomes to create nucleosome–nucleosome contacts. We will discuss the significance of the histone tails further when we look at the regulation of gene expression. Extensive investigation of the structure of nucleosomes has provided the basis for predicting how the chromatin fibre within the nucleus is formed, and how it coils up into the mitotic chromosome. In the representation shown here only a monomer of H2A and H2B can be observed, the other monomers being located at the back of the octamer. Instead, the 10 nm chromatin fibre is further packed into a thicker 30 nm fibre, which was originally called a solenoid. It is not clear whether the transition between the 10 nm fibre and the 30 nm fibre represents a physiological event or whether it merely occurs in vitro as a consequence of altering the salt concentration. The 30 nm fibre does, however, consist of numerous nucleosomes packed closely together, but the precise orientation and details of the structure are not clear. It has recently been suggested that the 30 nm fibre might adopt a compact helical zig-zag pattern with about four nucleosomes per 10 nm (Beard and Schlick, 1. The protein core is almost exclusively internal with the exception of the amino-terminal histone tails that extend out from the complex.
Generic sarafem 10mg free shipping. Women's Health Physiotherapy Birmingham.