
Alaska Bible College. I. Ernesto, MD: "Order Serophene - Safe online Serophene".
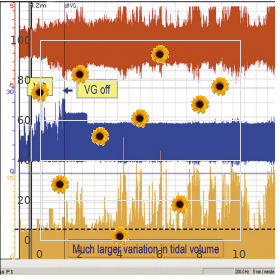
The mechanism is complex and may include vaso- motor order 50mg serophene with mastercard menstrual kits, autonomic (serotonergic brainstem systems) buy discount serophene 25mg online women's health clinic jersey city, Trigeminal Neuralgia and trigeminal nucleus dysfunction cheap generic serophene canada breast cancer 74 seconds. Treatment Trigeminal neuralgia (or tic douloureux ) is 16 is both abortive and prophylactic. Rapid abortive classically unilateral and usually located in treatment includes oxygen, sumatriptan (6 mg sub- the V2 or V3 distribution of the trigeminal nerve. It cutaneously), dihydroergotamine (1 mg intramus- has an electric shock quality lasting from seconds to cularly or subcutaneously), intravenous lidocaine minutes at a time and is ofen provoked by contact (100 mg), nasal butorphanol (1–2 mg), and sphe- with a discrete trigger. Patients are middle-aged and elderly, with include zolmitriptan nasal spray, dihydroergotamine a 2:1 female to male ratio. Prophylactic stem, cerebellopontine angle tumor, or multiple treatment may include β-adrenergic blockers, cal- sclerosis. The drug of choice for treatment is carbam- cium channel blockers, valproic acid, amitriptyline, azepine although it carries a risk of agranulocytosis. Phenytoin or baclofen may be added, particularly if patients do not tolerate the required doses of car- Cluster Headache bamazepine. More invasive treatments for patients Cluster headaches are classically unilateral and who do not respond to drug therapy include glycerol periorbital, occurring in clusters of one to three injection, radiofrequency ablation, balloon com- attacks a day over a 4- to 8-week period. The pain pression of the gasserian ganglion, and microvascu- is described as a burning or drilling sensation that lar decompression of the trigeminal nerve. The Chronic abdominal pain can have a variety of causes, headaches are typically episodic but can become and it is useful to distinguish between somato- chronic without remissions. Abortive treatments A diferential epidural block may help in elucidat- includes oxygen and sphenopalatine block. Lithium, ing the primary source but is time consuming and a short course of steroid medication, and verapamil may be difcult to interpret. Dosing Maximum Daily Analgesic Onset (h) Dose (mg) Interval (h) Dosage (mg) Salicylates Acetylsalicylic acid (aspirin) 0. Regardless of the be potentially both diagnostic and therapeutic (see agent selected, in most instances drug therapy Chapter 46). The patient with pain of visceral origin should be provided on a fxed time schedule rather may beneft from a celiac or splanchnic block. Anticonvulsants may be use- Cancer-related pain may be due to the cancerous ful (Table 47–14). Intrathecal drug delivery sys- lesion itself, metastatic disease, complications such tems may improve analgesia and, via a drug-sparing as neural compression or infection, or treatment efect, help decrease side efects associated with oral such as chemotherapy or radiation therapy. Numerous intrathecal agents tion, the cancer patient may have acute or chronic have been studied, and opioids have been utilized pain that is entirely unrelated to the cancer. The pain both alone and in combination with other medica- manager must therefore have a thorough under- tions. Ziconotide is a direct-acting N-type calcium- standing of the nature of the cancer, its stage, the channel blocker that may be helpful for refractory presence of metastatic disease, and treatments. It acts by decreasing the Cancer pain can be managed with oral analge- release of substance P from the presynaptic nerve sics in most patients. It does not lead to signifcant withdrawal oids (codeine and oxycodone) for moderate pain, conditions if abruptly discontinued. Relative Initial Dosing Opioid Onset (h) Potency Dose (mg) Interval (h) Codeine 0. Acetaminophen Acetaminophen (paracetamol) is an oral analge- Interventional Therapies sic and antipyretic agent that recently has become available in the United States as an intravenous Interventional pain therapy may take the form of preparation (Ofrmev) for inpatient use. It inhibits pharmacological treatment, nerve blocks with local prostaglandin synthesis but lacks signifcant antiin- anesthetics and steroid or a neurolytic solution, fammatory activity. Acetaminophen has few side radiofrequency ablation, neuromodulatory tech- efects but is hepatotoxic at high doses. The recom- niques, or multidisciplinary treatment (psychologi- mended adult maximum daily limit is 3000 mg/d, cal interventions, physical or occupational therapy, reduced from a previously recommended limit of or modalities such as acupuncture). Norepinephrine Serotonin Reuptake Reuptake Antimuscarinic Orthostatic Half-Life Daily Drug Inhibition Inhibition Sedation Activity Hypotension (h) Dose (mg) Amitriptyline (Elavil) ++ ++++ High High Moderate 30–40 25–300 Bupropion (Wellbutrin) Low Low Low 11–14 300–450 Citalopram (Celexa) 0 +++ Low Low Low 35 20–40 Clomipramine (Anafranil) +++ +++ High Moderate Moderate 20–80 75–300 Desipramine (Norpramin) +++ 0 Low Low Low 12–50 50–300 Doxepin (Sinequan) High High Moderate 8–24 75–400 Escitalopram 0 +++ Low Low Low 27–32 10–20 Fluoxetine (Prozac) 0 +++ Low Low Low 160–200 20–80 Imipramine (Tofranil) ++ +++ Moderate Moderate High 6–20 75–400 Nefazodone (Serzone) 0 + Low Low Low 2–4 300–600 Nortriptyline (Pamelor) ++ +++ Moderate Moderate Low 15–90 40–150 Paroxetine (Paxil) 0 +++ Low Low Low 31 20–40 Sertraline (Zoloft) 0 +++ Low Low Low 26 50–200 Trazodone (Desyrel) 0 ++ High Low Moderate 3–9 150–400 Venlafaxine (Effexor) + +++ Low Low Low 5–11 75–375 Prostaglandins sensitize and amplify nocicep- as a result, it has been taken of of the market in the tive input, and blockade of their synthesis results United States. All undergo hepatic metabolism orthopedic and gynecological surgery, respond very and are renally excreted. Teir analgesic action is limited by side The most common side efects of aspirin (ace- efects and toxicity at higher doses. All antidepressant medications undergo exten- Lamotrigine (Lamictal) 24 25–400 2–20 sive frst-pass hepatic metabolism and are highly Phenytoin (Dilantin) 22 200–600 10–20 protein bound. Available agents difer in their side efects (see Table 47–13), Valproic acid (Depakene) 6–16 750–1250 50–100 which include antimuscarinic efects (dry mouth, 1 Efficacy in pain management may not correlate with blood level. It has an elimination half-life of 8 h, is let efect does not appear to appreciably increase minimally metabolized by the liver, and is primarily the incidence of postoperative hemorrhage follow- excreted unchanged in the urine. It has a half-life of 12 h, is metabolized by the be used in children with varicella or infuenza infec- liver, and most of its metabolites are excreted in the tions because it may precipitate Reye’s syndrome. Tese medications efects include nausea, headache, dizziness, consti- demonstrate an analgesic efect that occurs at a dose pation, insomnia, hyperhydrosis, hot fashes, vomit- lower than that needed for antidepressant activity, ing, palpitations, dry mouth, and hypertension. The most com- spinal cord injury when administered by continuous monly used agents are fuphenazine, haloperi- intrathecal drug infusion. Teir of this medication has been associated with fever, therapeutic action appears to be due to blockade altered mental status, pronounced muscle spasticity of dopaminergic receptors in mesolimbic sites. Unfortunately, the same action in nigrostriatal pathways can produce undesirable extrapyramidal side efects, such as masklike facies, a festinating Corticosteroids gait, cogwheel rigidity, and bradykinesia. Some Glucocorticoids are extensively used in pain man- patients also develop acute dystonic reactions such agement for their antiinfammatory and possi- as oculogyric crisis and torticollis. Tey may be given topically, efects include akathisia (extreme restlessness) and orally, or parenterally (intravenously, subcutane- tardive dyskinesia (involuntary choreoathetoid ously, intrabursally, intraarticularly, or epidurally). Like antidepressants, many of these which difer in potency, relative glucocorticoid and drugs also have antihistaminic, antimuscarinic, mineralocorticoid activities, and duration or action. Excess glucocorticoid Antispasmodics & Muscle Relaxants activity can produce hypertension, hyperglycemia, Antispasmodics may be helpful for patients with increased susceptibility to infection, peptic ulcers, musculoskeletal sprain and pain associated with osteoporosis, aseptic necrosis of the femoral head, spasm or contractures. Patients multiple sclerosis, low back pain, and spastic diple- can also develop the physical features characteristic gia. Lidocaine is given by infusion over 5–30 min Many corticosteroid preparations are suspen- for a total of 1–5 mg/kg. Procaine, 200–400 mg, can sions, rather than solutions, and the relative par- be given intravenously over the course of 1–2 h, ticulate size of a given glucocorticoid suspension whereas chloroprocaine (1% solution) is infused at may afect the risk of neural damage due to arterial a rate of 1 mg/kg/min for a total of 10–20 mg/kg. Monitoring by qualifed medical personnel should Because of the relatively small size of its suspension include electrocardiographic data, blood pressure, particles, dexamethasone is becoming the preferred respiration, pulse oximetry, and mental status, and corticosteroid for injection procedures involving full resuscitation equipment should be immediately relatively vascular areas, such as the head and neck available. Anticonvulsant medications are useful for Patients who do not respond satisfactorily to 18 anticonvulsants but respond to intravenous local patients with neuropathic pain, especially tri- geminal neuralgia and diabetic neuropathy. Tese anesthetics may beneft from chronic oral antiar- agents block voltage-gated calcium or sodium chan- rhythmic therapy. Mexiletine (150–300 mg every nels and can suppress the spontaneous neural dis- 6–8 h) is a class 1B antiarrhythmic that is commonly charges that play a major role in these disorders. Pregabalin be applied to dry, intact skin, alternating 12 h on, (Lyrica) is a newer agent that has been approved for then 12 h of.
Spine J 3(2):106–117; discussion 117 replacement using ProDisc: report of two cases discount serophene uk menopause 62 years old. Spine surgery for symptomatic degenerative lumbar disc dis- (Phila Pa 1976) 30(6):655–660 ease: a systematic review of the literature serophene 50mg lowest price menstruation forecast. J Spinal Disord Cerebrospinal Fluid Leak 13(5):422–426 Hadani M buy serophene with a visa menstrual like cramps at 33 weeks, Findler G, Knoler N, Tadmor R, Sahar A, Shacked I (1986) Entrapped lumbar nerve root in Postoperative Neuritis pseudomeningocele after laminectomy: report of three cases. Diagnosis with heli- dimensional fast spin-echo magnetic resonance cal computed tomography. Neurol Res of patients who underwent laminectomy for lumbar 21(Suppl 1):S23–S26 stenosis: a prospective study. Radiographics 20(6):1665–1673 vial cyst formation: A possible consequence of liga- mentum favum excision. Epub 2011 Nov 1 Gossypiboma Is M, Karatas A, Akgul M, Yildirim U, Gezen F (2007) A Residual/Recurrent Tumors retained surgical sponge (gossypiboma) mimicking a paraspinal abscess. J Comput Assist Tomogr spinal cord ependymomas: outcome and prognostic fac- 15(6):1000–1003 tors. Spine (Phila Pa 1976) ing in utero closure of myelomeningocele: clinical 29(14):1535–1540 implications and follow-up fndings. Neurosurg Focus acrylate during percutaneous vertebroplasty and 15(3):E8 kyphoplasty. Neurosurgery local leakage of bone cement after percutaneous 32(3):384–394; discussion 394–395 kyphoplasty and vertebroplasty. Spine (Phila Pa 1976) 40(12):865–875 expandable meshed bag augmented with pedicle or facet screws for percutaneous lumbar interbody fusion. Spine tomography-guided epidural patching of postoperative J 8(2):367–373 cerebrospinal fuid leaks. Surg Technol Int 14:287–296 Imaging of Vascular 12 and Endovascular Surgery Daniel Thomas Ginat, Javier M. On the other hand, basal revascularization option for complex cerebrovas- collateral vessels often regress. Stenosis or fow replacement prior to planned vessel sacrifce occlusion of the bypass typically occurs at or near for treatment of complex and fusiform aneurysms the anastomosis (Fig. However, the presence of fow-related occipital artery can be anastomosed to the middle enhancement distally suggests that the vessel is cerebral artery (Fig. Postoperative angiography formed as part of complex aneurysm obliteration reveals good revascularization in the majority of and moyamoya disease primarily in adults. Indeed, the angiographic particular technique, favorable results are fndings of synangiosis are characteristic and achieved in nearly 90% of cases. The patient was managed medically surgery shows a left temporal microcraniotomy and tem- but recently developed repeated episodes of transient isch- poralis muscle fap with a superfcial temporal artery emic attacks to the left hemisphere. Consequently, an branch and fascial cuff (arrow) juxtaposed against the onlay external to internal carotid artery bypass with myo- brain surface. Specifcally, a direct anasto- imaged obtained by injection through the left common mosis was not feasible due to lack of adequately patent carotid artery 3 months after surgery (b) demonstrates cortical branches. Rather, the superfcial temporal artery small collateral vessels (encircled) communicating branch was placed over the brain surface along with its between the intracranial and extracranial arteries. In addition, the temporalis muscle faps were the temporal lobe cortex and temporalis muscle 12 Imaging of Vascular and Endovascular Surgery 633 Fig 12. Although the muscle wrap itself is often of muscle tissue was frst introduced by Cushing inconspicuous, it should not be confused with as a treatment of ruptured aneurysms. The tem- tumor or other abnormalities, such as hemor- poralis muscle is an accessible source of the nec- rhage, on imaging (Fig. Alternatively, muslin has also been wrap can resorb and allow aneurysm expansion used as a wrapping material. Other complications include infec- practice of wrapping aneurysms has declined in tion or foreign body reaction, if synthetic materi- popularity. Thus, the role of imaging following used as a last resort for treatment of aneurysms aneurysm wrapping is to evaluate for integrity of when endovascular stenting/embolization or sur- the wrap, aneurysm expansion or hemorrhage, gical clipping is not feasible. Although aneurysm images show left temporal craniotomy and interval place- clipping was planned, muscle wrap was instead performed ment of the muscle wrap, which appears as soft tissue because clipping posed signifcant risk of occlusion of the attenuation material surrounding the aneurysm and par- thalamic perforator or constriction of the left P1 segment. They consist of a ultrasound is routinely used to assess for cerebral hinged wire with parallel ends that are straight or vasospasm, but the modality has limited sensitiv- curved. These clips also produce con- demonstrate multifocal steno-occlusive lesions siderable beam-hardening artifact that can and areas of hemorrhage (Fig. In addition, variable Ultimately, catheter-based angiography has been amounts of the anterior clinoid process may be considered to be the historical gold standard to resected in order to access paraclinoid aneurysms diagnose vasospasm. Deeply positioned aneurysms can The incidence of recurrent aneurysms after be diffcult to attain for clipping, which can result complete clipping is approximately is low, but in aneurysm remnants. Incomplete clipping can this complication can lead to subarachnoid hem- present as increased hemorrhage shortly after orrhage and requires repeat clipping or endovas- clipping of ruptured aneurysms, for example, and cular intervention. It is also important to carefully can be addressed by endovascular embolization search for new aneurysms on postoperative scans, (Fig. Although the brain can be retracted since the annual rate of de novo aneurysm forma- in order to maximize the feld of view and access tion is about 0. These occur on average at for centrally located aneurysms, vascular injury about 10 years after surgery. Likewise, vessels adjacent to aneu- angiographic follow-up is warranted in patients rysms that have poor visibility can be inadver- with clipped aneurysms. However, seizure outcome optimal treatment option for arteriovenous mal- after resection of cavernous malformations is bet- formations and cavernous malformations. While ter when surrounding hemosiderin-stained brain the nidus of the arteriovenous malformation rep- also is removed, although this can be challenging resents the target of resection, the remaining when critical structures are involved (Fig. However, proximal ligation of the often transspatial and are often not amenable to supplying arteries alone can make subsequent complete surgical resection. However, when lym- embolization more diffcult and may rapidly lead phatic malformations compromise critical struc- to revascularization. For inoperable arteriove- tures, such as the airway, partial resection may be nous malformations that require treatment, ste- performed. This rate delineation of the residual tumor, which is treatment essentially results in thrombosis of the useful for planning subsequent additional surgery malformation. Obtaining necrosis can result, which may appear as a up-to-date imaging is particularly relevant since peripherally enhancing lesion with surrounding the lesions often evolve spontaneously, with new vasogenic edema (Fig. Postoperative axial T2-weighted (*) 12 Imaging of Vascular and Endovascular Surgery 643 12. Perhaps the most common complica- Microvascular decompression can be used to tion of microvascular decompression is recurrent effectively treat vascular loop syndromes, such symptoms related to suboptimal pledget posi- as trigeminal neuralgia and glossopharyngeal tioning (Fig.
The efect of sig- of the internal carotid artery generic 100mg serophene menopause underarm odor, external carotid artery best order serophene breast cancer encouragement, or both nal loss is typical for them buy discount serophene 50mg on line menstruation 9 dage, due to the fast turbulent blood of them, with cavernous sinus. The pathological vessels have low of arteriosinus anastomosis in cavernous sinus anastomosis signal in all modes. АG in coro- nal and lateral projections (a,b) demon- strate an abnormal drainage of blood into the dilated cavernous sinus and superior ophthalmic vein in early arterial phase. The clinical course cavernous and sphenoparietal sinuses, veins of dura mater, of the disease can be progressive, undulating and regressive. It reveals the sources of nus (possibly bilaterally) and the presence of multiple ways of blood supply and ways of outfow from cavernous sinus. All of them are flled with blood and are separated by sof tissue membranes with diferent thick- 3. Capillaries may lications in the literature with subarachnoid, intraventricular be present between the caverns. The peri- focal region is characterized by reactive changes of glia with Cavernous angiomas are observed in approximately 8−16% staining in yellow colour due to haemosiderin deposition in of all brain vascular malformation. Cavernous angioma (a) of a typical structure: vascular cavities are flled with erythrocytes and the walls consist of fbrous tissue (Mallory stain, magnifcation ×100). Marginal zone of cavernous angioma (b) on the border of hypoplastic brain tissue [hematoxylin−eosin (H&E) stain, magnifca- tion ×100]. Large calcinates in walls (c), stroma and in the cavity of cavernous angioma (b/w, H&E stain, magnifcation ×100). Hypointense rim from haemosiderin has a typical Cerebral angiography, as a rule, does not reveal any patho- appearance on T2-weighted images (Fig. In some cases the calcifca- riphery on T1- and especially on T2-weighted images are gener- tions may form the majority of the lesion (Fig. In these cases cysts and acute haemorrhages (hy- stages, and regions without thrombosis, can be identifed. CТ before (a,b) and afer (c) contrast enhancement demonstrates a small area of hyperdensity (arrow) with microcalcinates in the centre. Т1 (c,e) demonstrates areas of subacute haemorrhage (hyperintensity of methaemoglobin within cavities of the cavernous angioma) Cerebrovascular Diseases and Malformations of the Brain 317 Fig. Combination of hypo- and hyperintense signal is a sign of repeated haemorrhages Fig. Two microcav- reveal a large cavernous angioma with minimally present focal con- ernomas are additionally revealed in the right frontal area (e) 320 Chapter 3 Fig. Cavernoma is isointense (b) and afer contrast enhancement weakly accumulates in the afected zone (c) angiomas and are the most common vascular malformation a haemorrhage in the brain parenchyma (more ofen in the identifed at post-mortem examination (Okazaki 1989). Tat is why the term “occult cerebral vascular malformation” was introduced in the literature towards the end of the twen- 3. Venous channels are separated by normal brain pa- tiple small veins with characteristic shapes of “lion tail brush” renchyma. Haemorrhages are uncommon, but the risk of their or “Medusa head” is very well depicted during the late venous development exists. In 70% of cases the drainage is into the superfcial venous system, and subependymal drainage occurs in 22% of cases. Large veins usually have the appear- into a single, dilated venous structure and form venous an- ance of linear hypointense structures on T1- and T2-weighted gioma (Lasjaunias 1986). Venous malformations located in the brainstem or cerebellum have a slightly increased incidence of haemorrhage. As a rule, in the arterial phase there is no pathol- and periventricularly are drained into a single dilated transcortical ogy on angiograms. Fast fow in- Varicose dilatation of cerebral veins are seen mainly in asso- side the varices produces low signal. Ad- small veins fowing into a drainage vein ditional projections on Т1 (b,c) and T2 (d) allow to obtain additional Cerebrovascular Diseases and Malformations of the Brain 327 Fig. On Т2 (a) and Т1 without (b) and afer (c,d) con- the presence of a pathologically dilated vein draining into the supe- trast enhancement the drainage vein of venous angioma is indicated rior sagittal sinus (e,f) Fig. Abnormal varicose dilation of veins is seen Cerebrovascular Diseases and Malformations of the Brain 329 Fig. Springer Verlag Ber- Astrup J, Simon L, Siesjo B (1981) Tresholds of cerebral ischaemia: lin pp. Neurosurgery 82:167-179 330 Chapter 3 Borisch I et al (2003) Preoperative evaluation of carotid artery steno- Garcia J, Mitchem H, Briggs L et al. Neuroradiology 37:262–266 Goddard A, Mendelow A, Birchall D (2001) Carotid stenosis in the Brunereau L et al. Neuroimaging Clin N Am 8:295–321 Hochmuth A, Spetzger U, Schumacher M (2002) Comparison of Cognard C, Gobin Y, Pierot L et al (1995) Cerebral dural arterio- three-dimensional rotational angiography with digital subtrac- venous fstulas: clinical and angiographic correlation with a revis- tion angiography in the assessment of ruptured cerebral aneu- ited classifcation of venous drainage. Cavernous mal- Ernemann U et al (2000) 3D angiography in treatment planning of formations. Stroke Konovalov A et al (2001) Haemorrhage and silent vascular malfor- 30:1751–1758 mations of the brainstem. Feb 47(2):138-43 (review) Lasjaunias P, Alvarez H, Rodesch G et al (1996) Aneurysmal malfor- Furst G, Hofer M, Steinmetz H et al. Neuroimaging Gannushkina I (1975) Physiology and pathophysiology of cerebral Clin N Am 13:139–152 blood supply. Radiology 211:775–780 telangiectasia: a spectrum within a single pathological entity. Neurosurgery carotid plaque composition, morphology and neurological symp- 80:217–223 toms. Radiology 93:1071–1078 brain and certain compensatory vascular reactions in carotid- cavernous anastomoses. Nov-Dec (6):12–7 (in russian) 3(5):218–225 Picard L, Bracard S, Moret J et al (1987) Spontaneous dural arterio- Suzuki J (1986) Moyamoya disease. Arch pl):162 (in russian) Neurol 20:288–299 Pollock B, Flickinger J, Lundsford L et al. J Cereb ogy 15:225-237 Blood Flow Metab 19:99–108 Yamamoto K, Nogaki H, Takase Y et al. Georg Tieme Verlag, Vereshchagin N et al (2002) Stroke: principles of diagnosis, treatment, Stuttgart and prevention. Annually, up to 11 per 100,000 new cases of 334 Chapter 4 Histological Classification of Tumours Histological Classification of Tumours of the Central Nervous System of the Central Nervous System 1. Sixty percent of all cases Unlike adults, tumours originating from neuroglia are were tumours originated from neuroepithelial tissue. Approximately two thirds of brain gliomas constituted the largest group among neuroepi- all intracranial neoplasms are benign forms.
In the last two decades order serophene us womens health blog, there has been a steady stream of research dedicated to develop peripherally restricted opioid receptor agonist molecules for this purpose buy serophene 25mg with amex menstruation vs pregnancy. As of date buy line serophene womens health questions, there are no specifically approved peripherally restricted opioid molecules available solely for peripheral analgesic application. Analgesia after topical application of opioids has been demonstrated in patients with various types of acute (e. They lacked side effects similar to that seen with morphine, at the same time being effective clinically. These two compounds were shown to be peripherally selective κ receptor agonists with analgesic and anti- inflammatory properties. The first is the use of centrally active agonists (the prototype being morphine) in peripheral locations for peripheral opioid action, e. The best example of this class is use of loperamide to attenuate neuropathic pain. The third is the development of specific compounds with peripheral and selective µ receptor agonist action. It acts on peripheral opioid receptors and does not cross blood brain barrier due to its large size. These peripheral analgesic actions are modulated by action on the peripheral opioid receptors. These actions of opioids on peripheral receptors gets enhanced in presence of inflammation, which releases propeptide substances like corticotropin releasing hormone and cytokines. These peripheral opioid agonists have advantage of avoiding potential and dangerous adverse effects that usually occurs because of action on central nervous system when these opioids are given in systemic route, e. Substantial research work is going on to find out the effective peripherally acting opioids, which ideally will replace systemic opioids in future and thereby not only reduce the risk of addiction but also harmful side effects. Opiates inhibit the discharges of fine afferent units from inflamed knee joint of the cat. Modulation of peripheral sensory neurons by the immune system: implications for pain therapy. Inhibition by spinal mu- and delta-opioid agonists of afferent-evoked substance P release. Emerging roles for G protein-gated inwardly enhances axonal transport of opioid receptors in the sciatic nerve and increases their density in the inflamed tissue. Opioids inhibit purinergic nociceptors in the sensory neurons and fibres of rat via a G protein- dependent mechanism. Mu-opiate receptor and Beta- endorphin expression in nerve endings and keratinocytes in human skin. Mu opioid receptor expression is increased in inflammatory bowel diseases: Implications for homeostatic intestinal inflammation. Activation of delta opioid receptors induces receptor insertion and neuropeptide secretion. Morphine and pain-related stimuli enhance cell surface availability of somatic delta-opioid receptors in rat dorsal root ganglia. Peripheral delta opioid receptors require priming for functional competence in vivo. Opioid receptors and opioid peptide producing leukocytes in inflammatory pain—basic and therapeutic aspects. Opioids from immunocytes interact with receptors on sensory nerves to inhibit nociception in inflammation. Opioid peptide–expressing leukocytes: Identification, recruitment, and simultaneously increasing inhibition of inflammatory pain. Subcellular pathways of beta-endorphin synthesis, processing, and release from immunocytes in inflammatory pain. Effects of peripheral nerve ligation on expression of mu-opioid receptor in sensory ganglion neurons: an immunohistochemical study in dorsal root and nodose ganglion neurons of the rat. Neurokinin-1 receptor antagonists inhibit the recruitment of opioid-containing leukocytes and impair peripheral antinociception. Sympathetic activation triggers endogenous opioid release and analgesia within peripheral inflamed tissue. Painful inflammation- induced increase in μ-opioid receptor binding and G-protein coupling in primary afferent neurons. Inflammation enhances peripheral muopioid receptor- mediated analgesia, but not mu-opioid receptor transcription in dorsal root ganglia. Tappe-Theodor A, Agarwal N, Katona I, Rubino T, Martini L, Swiercz J, Mackie K, Monyer H, Parolaro D, et al. The other side of the opioid story: modulation of cell growth and survival signaling. Analgesic effects of peripherally administered opioids in clinical models of acute and chronic inflammation. Double-blind doseresponse multicenter comparison of fedotozine and placebo in treatment of nonulcer dyspepsia. Efficacy of peripheral kappa agonist fedotozine versus placebo in treatment of irritable bowel syndrome. Analgesia from a peripherally active kappa-opioid receptor agonist in patients with chronic pancreatitis. Intraarticular morphine, bupivacaine, and morphine/bupivacaine for pain control after knee videoarthroscopy. A novel molecule (frakefamide) with peripheral opioid properties: The effects on resting ventilation compared with morphine and placebo. It has a highly selective action at α-2 adrenoceptor and so possesses sympatholytic, sedative, amnestic, and analgesic properties, notably without respiratory depression. It potentiates the effects of anesthetic drugs and hence, is being studied intensely as an adjunct to many anesthetic techniques. Amino acid composition in these three isoreceptors is 70–75% and they bind α-2 agonists and antagonists with similar affinities. Agonism at the α-2a receptor produces sedation, hypnosis, analgesia and sympatholysis; α-2b promotes analgesia at spinal cord sites, causes vasoconstriction in peripheral arteries and suppresses shivering. Action via α-2c receptor results in modulation of cognition, sensory processing and mood and stimulant-induced locomotor activity. There is suppression of neuronal firing with efflux of potassium through calcium-activated potassium channels and an inhibition of calcium entry into calcium channels at the nerve terminals. Major side effects observed following the infusion are bradycardia and hypotension. Inhalational agents decrease blood pressure at the expense of vasodilatation and reflex tachycardia. This bradycardia was not symptomatic and also did not warrant any advanced hemodynamic support. Concomitant perioperative use of beta blockers, which may act synergistically, increases the risk of stroke and death. Drug did not compromise airway although some patients required midazolam to maintain Ramsay 2. So, requirements of muscle relaxant and hence the risk of residual muscle weakness during emergence decreases.