
Saint Xavier University. U. Campa, MD: "Buy Top Avana online in USA - Proven Top Avana online OTC".
X The purpose of the research will provide an indicator to the most appropriate methods cheap 80 mg top avana amex impotence and diabetes 2. X You should think about your personality buy top avana pills in toronto erectile dysfunction over 70, strengths and weakness cheap top avana amex erectile dysfunction 60784, likes and dislikes when choosing re- search methods. This will help you to become more familiar with your topic and intro- duce you to any other research which will be of benefit to you when you begin your own project. PRIMARY RESEARCH AND SECONDARY RESEARCH There are two types of background research – primary re- search and secondary research (see Table 2). Primary re- search involves the study of a subject through firsthand observation and investigation. This is what you will be doing with your main project, but you may also need to conduct primary research for your background work, especially if you’re unable to find any previously pub- lished material about your topic. Primary research may come from your own observations or experience, or from the information you gather personally from other people, as the following example illustrates. I had noticed how some children didn’t fit the classic description of a truant and I wanted to find out more as I thought it might help me to deal with some of the problems children were experiencing. So I guess you’d say my own experience provided me with some initial data. Then I decided to go and have a dis- cussion with some of my colleagues and see if they’d noticed anything like me. It was really useful to do this because they helped me to think about other things I hadn’t even thought of. One of them told me about a new report which had just come out and it was useful formetogoandhavealookatitasitraisedsome of the issues I was already thinking about. Actually this made me change the focus of my work a little because I soon found out that there had been a lot of work on one area of what I was doing, but not so much on another area. It was really useful to have done this before I rushed into my research as I think I might have wasted quite a bit of time. In the above example, Jenny mentions a recently pub- lished report which she has read. This is secondary re- search and it involves the collection of information from studies that other researchers have made of a subject. The two easiest and most accessible places to find this informa- tion are libraries and the internet. However, you must re- 42 / PRACTICAL RESEARCH METHODS member that anybody can publish information over the internet and you should be aware that some of this infor- mation can be misleading or incorrect. Of course this is the case for any published information and as you develop your research skills so you should also develop your criti- cal thinking and reasoning skills. What motives did the publishers have for making sure their information had reached the public domain? Using web sites By developing these skills early in your work, you will start to think about your own research and any personal bias in your methods and reporting which may be present. The web sites of many universities now carry information about how to use the web carefully and sensibly for your research and it is worth accessing these before you begin your background work. When you’re surfing the net, there are some extra precau- tions you can take to check the reliability and quality of the information you have found: X Try to use websites run by organisations you know and trust. X Check the About Us section on the web page for more information about the creator and organisation. X Use another source, if possible, to check any informa- tion of which you are unsure. For example, if you’re interested in medical information you can check the HOW TO CONDUCT BACKGROUND RESEARCH / 43 credentials of UK doctors by phoning the General Medical Council. X You should check the national source of the data as in- formation may differ between countries. X For some topics specific websites have been set up that contain details of questionable products, services and theories. Interlibrary loans If you are a student your institutional library will prob- ably offer an interlibrary loan service which means that you can access books from other university libraries if they are not available in your library. This is a useful service if, when referencing, you find that a small amount of infor- mation is missing (see Example 5 below). EXAMPLE 5: GILLIAN Nobody told me the importance of keeping careful re- cords of my background research. I just thought it was something you did and then that was it, you got on with 44 / PRACTICAL RESEARCH METHODS your own research and forgot about what you’d done. Of course then I had to write my report and in the ‘background’ section I wanted to include loads of things I’d read when I first started the work. Even then I still forgot to write down the name and location of the publisher, so I had to go back to them again. My advice would be to look at how bibliographies are structured and imprint that in your brain so you don’t forget anything. Keeping records When you begin your background research, keep accurate records of what data was gathered from which source as this will save you plenty of time and frustration later, especially when you come to write your research proposal, or final report. A useful way to organise your background research is to have two files – one for primary research and one for secondary research. Each file can be divided into topics with the relevant notes slotted into each. Primary research For the primary research file, notes from each contact can be separated by a contact sheet which gives the name of the person, the date and time you met and a contact num- ber or address. Secondary research In the secondary research file, each page of notes can be headed by details of the publication in the same format that will be used in the bibliography – author and initials; date of publication; title of publication; place of publica- HOW TO CONDUCT BACKGROUND RESEARCH / 45 tion and publisher. If it is a journal article, remember to include the name of the journal; the page numbers of the article and the volume and number of the journal. It is also useful to include the location of this publication so that it can be found easily if needed again (website or li- brary shelf location). TABLE 2: SOURCES OF BACKGROUND INFORMATION PRIMARY SECONDARY Relevant people Research books Researcher observation Research reports Researcher experience Journal articles Historical records/texts Articles reproduced online Company/organisation records Scientific debates Personal documents (diaries, etc) Critiques of literary works Statistical data Critiques of art Works of literature Analyses of historical events Works of art Film/video Laboratory experiments SUMMARY X There are two types of background research – primary and secondary research. X Primary research involves the study of a subject through firsthand observation and investigation. X Secondary research involves the collection of informa- tion from studies that other researchers have made of a subject. X Any information obtained from secondary sources must be carefully assessed for its relevance and accu- racy. X Notes from primary and secondary sources should be carefully filed and labelled so that the source can be found again, if required. X When noting details for books, reports or articles which may appear in the final report, include all the details which would be needed for the bibliography. By now you should have decided what type of peo- ple you need to contact.
He has Brigham Hospital cheap 80 mg top avana with visa erectile dysfunction medication otc, where he received his post- also been a consultant to many of the major hos- graduate education in surgery and remained as a pitals in Boston discount top avana 80 mg with amex impotence cures. Furthermore top avana 80 mg on line erectile dysfunction medications cost, he has served on member of the staff until his retirement in 1974. In 1978, he was editor of the Year Book 285 Who’s Who in Orthopedics of Sports Medicine. He received an honorary membership in the American Orthopedic Associ- ation for Sports Medicine in 1976, and was cited as “Sportsman of the Year” in 1978. During the period from 1977 to 1978, he was president of the Harvard Medical Alumni Association. Quigley has made numerous contributions to the art and practice of orthopedic surgery, but his approach to the management of the frozen shoulder and the development of a procedure to stabilize the knee utilizing the popliteal muscle deserve special attention. Quigley has served as a role model for students and residents for more than four decades. He has been a superb teacher, perhaps in part owing to his acting talents, but also because of his knowledge and surgical abilities. REYNOLDS especially athletes, students, and residents, and he has encouraged the scholarly activities of numer- 1908–1986 ous surgical and orthopedic residents. He enrolled Whether on rounds or in the operating room, in Washington University in 1926 and received a Dr. Quigley has evidenced the ability to recognize Doctor of Medicine degree in 1934. In surgical house officer at Barnes Hospital under the care of patients, the education of students and the supervision of Dr. In 1942, Fred entered active duty with the References United States Army and in 1943 was transferred to England. Quigley TB (1954) Checkrein shoulder: A type of General Hospital in 1944, he met Lieutenant “frozen” shoulder. Diagnosis and treatment by Phyllis Terry, a nurse who was assigned to the manipulation and ACTH or cortisone. Southmayd W, Quigley TB (1978) The forgotten became chief of orthopedic surgery at Gardiner popliteus muscle: Its usefulness in correction of anteromedial rotatory instability of the knee. Clin Orthop 130:218 civilian life, after achieving the rank of lieutenant colonel in 1946. Key in practice, and resumed his affil- iation with Washington University and the Barnes Hospital. He developed an interest in basic research and wrote articles on the banking of bone, experimental fracture healing, arthroplasty, and the spine. In 1961, Fred coauthored the seventh edition of Fractures, Dislocations and Sprains, the definitive textbook on fractures for that time. Carl Moyer to join the full-time faculty at 286 Who’s Who in Orthopedics Washington University, and in 1956 he became and teachers than he was. It is unlikely that any professor and chief of the Division of Orthopedic ever were. He subsequently developed an academic large man, but he was one of the giants of program that had ten full-time faculty members orthopedics. Louis on October 10, attracted residents and faculty from the entire 1986, from carcinoma of the pancreas. He retired as chairman in 1972 and to Phyllis, he left three children: Mary Ann Krey, became professor emeritus in 1976. Reynolds Chair of Orthopedic Surgery was created at Washington University in 1979 from contributions by his friends, students and patients. Fred became active in the American Academy of Orthopedic Surgeons, serving as chairman of the Instructional Course Committee from 1959 to 1961, chairman of the Committee on Graduate Education from 1961 to 1964, and editor of the Instructional Course Lectures and president in 1965. He was president of the Clinical Orthope- dic Society in 1960, and he was elected to the American Orthopedic Association. In addition to being a member of the American Board of Ortho- pedic Surgery and of state and local orthopedic and surgical societies, Fred was president of the St. Louis Orthopedic Society and of the Clinical Orthopedic Society and served on study sections of the National Institutes of Health and the editorial board of The Journal of Bone and Joint Surgery, and was a founder and first president of Frederic W. His father was an Episcopalian Fred considered his major responsibility to minister who became the bishop of Pennsylvania. His greatest Washington, DC, where he received a rigorous quality as a teacher was his uncompromising classical education. He was his own severest degree from Harvard University in 1928, he critic, a quality he taught by example to those attended Oxford University, which awarded him around him. He had no patience for stupidity or an additional bachelor’s degree and a master’s laziness. Fred’s advice to residents, whether they degree from the school of medicine. He then entered military service (an experience he thought returned to the United States and obtained his would be valuable) or practice, was the same: medical degree from Harvard University in 1934. His postgraduate training embraced a broad Fred was a master surgeon and a careful and experience in research and the basic sciences and thoughtful physician. In 1941, he joined the faculty of superficially, he was a crusty, grumpy, taciturn Harvard University Medical School, where he man. But those who were privileged to be asso- remained until 1947, with a hiatus as a medic in ciated with him knew him as a caring, compas- World War II. While in the service, Rhinelander sionate, highly skilled physician, teacher, and became chief of orthopedics at the Letterman friend. His wish for his residents was that they General Hospital in San Francisco. His experi- should be better physicians, surgeons, scholars, ence with the use of iliac bone grafts in the treat- 287 Who’s Who in Orthopedics ment of ununited fractures was substantial. After attending Harvard University, Boston, MA, he leaving the service, he entered private practice in studied medicine at the College of Physicians and San Francisco and had a clinical appointment on Surgeons, in New York City. After receiving his the faculty of the University of California in San medical degree in 1939, he interned and served a Francisco. In 1955 he joined the faculty of Case year of general surgery residency in the Brooklyn Western Reserve University School of Medicine, Hospital. Shortly after beginning his orthopedic where he remained, retiring as professor emeritus residency at the Presbyterian Hospital in New in 1972. It was while he was in Cleveland that York City, his training was interrupted by World Rhinelander did his intensive study of the micro- War II. Robinson served in army hospitals in the circulation in bone and the effects of operative United States and in the South Pacific. After his retire- of his discharge he was the commanding officer ment, he moved to Little Rock, AR, where he and chief of surgery of the 90th Field Hospital served on the faculty of the University of in Leyte, Philippine Islands. In 1979, Rhinelander returned to in 1946, he resumed his orthopedic training at California, where he was appointed research pro- Strong Memorial Hospital in Rochester, NY. It was his The quality of Rhinelander’s work on the experience in England that first stimulated his microcirculation of bone was recognized by the interest in surgery of the spine.
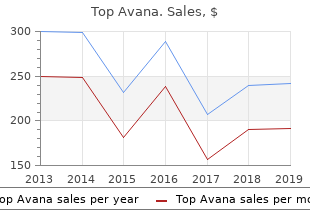
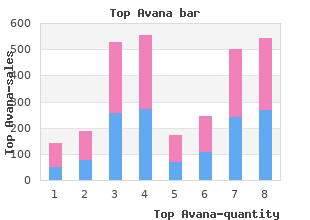
False Bittersweet (American Bittersweet). Top Avana.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96296
It was given to a packed audience in the advanced course upper lecture room of the Kongress Halle in Davos cheap top avana 80mg with visa erectile dysfunction medications cost. The par- ticipants were in awe of his surgical technique and ability to reduce difficult and extensive fractures order top avana overnight delivery impotence 1. His presentation included numerous examples of anatomic reduction of complex associated acetab- ular fractures with excellent 10–20 year results cheap top avana 80mg visa erectile dysfunction risk factors. These radiographs demonstrated long, twisted reconstruction plates curving around areas of the pelvis (that the majority of the course participants had never visualized), creating a singular educa- 191 Who’s Who in Orthopedics tional experience and a standing ovation. Emile These latter two textbooks are the primary continued to be an immutable participant in the sources of information on surgery of the acetab- advanced courses in Davos and participated in ulum in the English literature and are considered countless AO courses throughout the United the “Bibles” of acetabular surgery. His unique personal- resulted in a complete transformation of our ity and energy were legendary, and he was always understanding and treatment of fractures of the available to answer the most trivial question from acetabulum. His passion and love of Emile Letournel was born on the French island teaching extended worldwide as his results of St. Pierre et Miquelon, situated between New became universally acknowledged. Emile’s per- Foundland and Nova Scotia, on December 4, sonality and professional camaraderie were 1927. He never spoke English while growing up quintessential Letournel, and his dedication to and after finishing secondary school in St. Pierre teaching his techniques to conferences all over the he obtained a scholarship to the French Institute world was the underlying virtue of this great man. During this time period, the war There are many instances in the history of in Europe was at a climax and for safety reasons orthopedic surgery in which an individual the French Institute was moved to Hullswater surgeon has made a significant contribution to a Lake, Cumberland Scotland, near Edinburgh for particular area of surgery that has stood the test the duration of the war. There are very few instances of a sur- et Miquelon alone at the age of 16 on July 27, geon contributing to the specialty of orthopedic 1944 to cross the Atlantic and attend school in and trauma surgery in the complete and life- Scotland. At the time of his departure, he did not long manner that was characteristic of Emile speak English and had never seen a train or a big Letournel. Pierre, “Le Cap tion of the correct radiographic and anatomic Bleu,” to Nova Scotia (24 hours) and then to diagnoses of acetabular fractures and progressed Montreal by train (36 hours). He left Montreal on to a logical classification of these injuries into ele- August 7, 1944 in one of the largest convoys of mentary and associated fracture types. On his ship, continued with development of two major surgi- “The Jamaica Planter,” no one spoke French and cal exposures, reduction techniques, instruments all his personal belongings were confiscated until and implant designs used in every operating the boat arrived in Scotland 28 days later. Though there have studied for a year at the French Institute and been refinements over time and contributions by received his Premier Bacalaureat. After the war other authors in the field, Letournel’s original he left England for France, where he studied at description, diagnosis, classification and surgical the Lycee Chaptal and received his Second techniques have remained the ubiquitous standard Bacalaureat. He was admitted to the Faculty of of care of acetabular fractures for the past 25 Medicine of Paris from 1946 to 1960 and became years. His thesis published in 1961, a postgraduate position to continue his education. Etude d’une serie de 75 This process required the applicant to visit all cas,” contained the initial description of the clas- professors who were offering training positions. Pierre, Emile had no letters of Robert Judet and has achieved worldwide accept- support to compete adequately for an orthopedic ance. A friend suggested he contact Professor education in the understanding of the complex Robert Judet and he did this out of desperation nature of acetabular fractures. The major textbooks on acetabular surgery, all with meeting with Robert Judet was very brief. Professor Judet asked him where he and the third, Fractures of the Acetabulum in came from and Emile responded “St. The 6-month position lasted 12 months and found contributions to orthopedic surgery that Emile subsequently became Judet’s assistant. Professor Letournel to associate professor and finally professor in qualified uniquely for this honor as he was still 1970. He became head of the Department of alive when the commission was given to pay Orthopedic Surgery at the Centré Medico tribute to his life achievements in fracture surgery. Chirurgical de la Port de Choisy in southeast Unfortunately, he died 2 weeks before this journal Paris. He remained at the Choisy hospital until his was published with his dedication issue. In addition to his interest in acetabular and rugged and energetic and he lived life with great pelvic fractures, he performed over 6,000 total hip eagerness and excitement. His mere presence in arthroplasties, developed implant designs and sur- the operating theater created movement. As he gical techniques for management of calcaneal would scrub for surgery, his intensity to take on fractures and had extensive expertise in the sur- his worthy fracture adversary would bubble forth gical treatment of bone infection. His position at as he would review in his mind the preoperative Choisy provided him an unlimited exposure to plan of surgical approach and internal fixation. His distinctive vocal tal, and Professor Letournel never charged a commentary (always in French) on a particularly surgeon’s fee to any patient throughout his entire stubborn fragment reduction or repeated failed career at Choisy for his services. He was admit- surgical maneuver or the worthlessness of a par- ted to the French Academie de Medicine et ticular instrument to perform its function would Chirurgie in 1981 and received the “Legion create absolute silence from the operating theater d’Honneur” from President Mitterrand of France staff until a universal sigh of relief would resound in 1988. These honors were very special to Emile throughout the room when he was finally satisfied and were public recognition of his stature in with his reduction. Of special mention is Profes- French medicine and his accomplishments in the sor Letournel’s most trusted medical assistant, field of orthopedic trauma surgery. Following Remy Ser, who was the master of the Judet frac- his death, the elected officials of St. He could position any extremity on the Miquelon passed a resolution naming a street on fracture table into the desired position during the the island of his birth, “Emile Letournel. Remy Ser was an extremely dedicated who have been able to study with him at the professional and stayed with Emile for over 15 “Letournel School of Acetabular Surgery” gained years until the day he died. He was an integral tremendous insight into his diagnostic and surgi- part of the Letournel team perpetuating the cal acumen and the steadfastness with which he excellence that was the hallmark of Professor pursued every acetabular fracture to obtain “the Letournel’s surgery. He would continually Clinical Orthopedics and Related Research, ded- vocalize to himself all the possibilities and con- icated to Professor Letournel and his significant sequences of his technique while performing his contributions to orthopedic surgery. His genius had an enormous 193 Who’s Who in Orthopedics ability to comprehend spacial relationships, leading him to understand quickly the complexi- ties of a particular fracture and develop a plan of reduction based on his extensive experience. He was a masterful surgeon who knew well his abil- ities and limitations. He lived for the difficult trial, whether it was in the operating room or performing the ritualistic decapitation of a bottle of Dom Perignon with a saber, he was always the same wonderful man. His admirers encompassed the entire world of orthopedic and trauma surgery. His presentations were legendary and as uncommonly entertain- ing as his own form of English (an ingenious Letournel dialect), which created within the audience a profound awareness of the complexity Jacques LEVEUF of acetabular fractures and the importance of his 1886–1948 pioneering original and lifelong contributions to acetabular fracture surgery. This remarkable individual was not enormous Leveuf was born in Limoges and studied in the in physical stature, but he was immense in per- School of Medicine in Paris. He was hap- intern appointments he was for many years an piest in the operating theater struggling with a assistant in the surgical clinic of Pierre Delbet. He difficult fracture or enjoying personal moments worked with Delbet in the early attempts to nail with his loved ones and close friends.
Imaging of the cord order 80 mg top avana with mastercard young husband erectile dysfunction, ideally with MRI cheap top avana 80 mg line impotence lotion, may be helpful in defining the cause of myelopathy discount top avana 80mg online erectile dysfunction nitric oxide. London: BMJ Publishing, 1997: 272-294 Tartaglino LM, Flanders AE, Rapoport RJ. Seminars in Ultrasound, CT, and MRI 1994; 15: 158-188 Cross References Brown-séquard syndrome; Lower motor neurone (LMN) syndrome; Paraparesis; Proprioception; Sacral sparing; Suspended sensory loss; Upper motor neurone (UMN) syndrome; Vibration Myerson’s Sign - see GLABELLAR TAP REFLEX Myoclonus Myoclonus is involuntary, “shock-like,” muscle jerking, arrhythmic more often than regular, of central nervous system (CNS) origin. Multiple irregular asynchro- nous myoclonic jerks may be termed polymyoclonus. Myoclonus may be characterized in several ways: ● Clinical classification (by observation, examination): Spontaneous Action or intention: following voluntary action; may be elicited by asking patient to reach out to touch the examiner’s hand Reflex, stimulus-sensitive: jerks produced by somatesthetic stimulation of a limb, in response to loud noises ● Anatomical/pathophysiological classification (by electrophysio- logical recordings): Cortical Subcortical/reticular Propriospinal/segmental ● Etiological classification: Physiological, e. Periodic limb movement disorder or periodic leg movements of sleep, frequently found in association with restless legs syndrome, is sometimes called “nocturnal myoclonus. Drugs useful in the treatment of myoclonus include clonazepam, sodium valproate, primidone, and piracetam. These may need to be given in combination to suppress severe action myoclonus. Advances in Clinical Neuroscience & Rehabilitation 2003; 3(5): 20,22 Caviness JN. Mayo Clinic Proceedings 1996; 71: 679-688 Marsden CD, Hallett M, Fahn S. London, Butterworth, 1982: 196-248 Obeso JA, Artieda J, Rothwell JC, Day B, Thompson P, Marsden CD. Brain 1989; 112: 765-777 Cross References Asterixis; Chorea, Choreoathetosis; Fasciculation; Hiccups; Jactitation; Myokymia; Palatal myoclonus; Tic; Tremor Myoedema Myoedema, or muscle mounding, provoked by mechanical stimuli or stretching of muscle, is a feature of rippling muscle disease, in which the muscle contractions are associated with electrical silence. Muscle and Nerve 2002; Suppl 11: S103-S107 Myokymia Myokymia is an involuntary, spontaneous, wave-like, undulating, flickering movement within a muscle (cf. Myokymia is thus related to neuromyotonia and stiffness, since there may be concurrent impair- ment of muscle relaxation and a complaint of muscle cramps. Facial myokymia is a rare facial dyskinesia, possibly related to disinhibition of the facial (VII) nerve nucleus by focal pontine lesions (tumor, demyelination). Boston: Butterworth, 1994: 373-405 Cross References Fasciculation; Myotonia; Neuromyotonia; Stiffness Myopathy The term myopathy means a primary disorder of muscle causing wast- ing and/or weakness in the absence of sensory abnormalities. Clinically, myopathic processes need to be differentiated from neu- ropathies, particularly anterior horn cell diseases and motor neu- ropathies, and neuromuscular junction disorders. Generally in primary muscle disease there are no fasciculations, reflexes are lost late, and phenomena such as (peripheral) fatigue and facilitation do not occur. Myopathies may be subdivided according to the clinical pattern of weakness, and/or their etiology: ● Proximal: Affecting shoulder abductors, hip flexors predominantly: Inflammatory: polymyositis, dermatomyositis Progressive muscular dystrophies: Duchenne, Becker, limb- girdle, facioscapulohumeral (FSH) Metabolic: acid-maltase deficiency; thyroid dysfunction, Cushing’s syndrome Nonmetastatic feature of malignant disease. Philadelphia: Lippincott Williams & Wilkins, 2002: 623-641 Cross References Atrophy; Bulbar palsy; Camptocormia; Dropped head syndrome; Facial paresis; Fatigue; Gowers’ sign; Paradoxical breathing; Wasting; Weakness Myorhythmia Myorhythmia is an involuntary movement disorder characterized by rhythmic contraction (1-3 Hz) of muscles producing a coarse tremor, which may affect limbs, face, palate, head, jaw, neck, tongue, eyes or trunk. They are associated with brainstem or thalamic vascular dis- ease, trauma, alcohol-related nutritional deficiency, phenytoin intoxication, Hashimoto’s encephalopathy, paraneoplasia, and Whipple’s disease. Although very rare, oculomasticatory myorhythmia is of diagnos- tic importance since it is pathognomonic for Whipple’s disease of the nervous system. Characteristically there is also convergent-divergent pendular nystagmus with synchronous rhythmic movement of the mouth, tongue, jaw and sometimes proximal and distal skeletal mus- cles. The neurological manifestations of Whipple’s disease are protean, and include dementia, ataxia, supranuclear ophthalmoplegia (with sparing of the pupils), seizures, myoclonus, nystagmus and psychosis. Treatment is with antibiotics, usually a two-week intravenous course of trimethoprim-sulphamethoxazole or ceftriaxone followed by oral treatment for one year. Sodium valproate may be helpful for the invol- untary movements which do not respond to antibiotics. Journal of Neurology, Neurosurgery and Psychiatry 2000; 68: 2-5 Masucci EF, Kurtzke JF, Saini N. Brain 1984; 107: 53-79 Simpson DA, Wishnow R, Gargulinski RB, Pawlak AM. Oculofacial- skeletal myorhythmia in central nervous system Whipple’s disease: additional case and review of the literature. Movement Disorders 1995; 10: 195-200 Cross References Ataxia; Dementia; Myoclonus; Nystagmus Myotonia Myotonia is a stiffness of muscles with inability to relax after volun- tary contraction (action myotonia), or induced by electrical or mechanical (e. A similar clinical phenomenon of slow muscle relaxation may be observed in other circumstances, for example hypothyroidism, but without the characteristic EMG findings of myotonia, hence this is labeled as pseudomyotonia. Paramyotonia is myotonia exacerbated by cold and exertion (paradoxical myotonia). Recognized causes of myotonia include: ● myotonic dystrophy (myotonia dystrophica; myotonic dystrophy type 1) ● hyperkalaemic periodic paralysis ● myotonia congenita (autosomal dominant Thomsen’s disease, autosomal recessive Becker’s myotonia) ● K+-aggravated myotonia ● Schwartz-Jampel syndrome (chondrodystrophic myotonia) ● proximal myotonic myopathy (PROMM; myotonic dystrophy type 2) Mutations in genes encoding voltage-gated ion channels have been identified in some of the inherited myotonias, hence these are chan- nelopathies: skeletal muscle voltage-gated Na+ channel mutations have been found in K+-aggravated myotonia, and also paramyotonia con- genita and hyperkalaemic periodic paralysis. Chloride (Cl−) channel mutations have been identified in myotonia congenita. Current Opinion in Neurology 2002; 15: 545-552 Cross References Neuromyotonia; Paramyotonia; Percussion myotonia; Pseudomyotonia; Stiffness; Warm-up phenomenon; Woltman’s sign - 209 - N Narcolepsy, Narcoleptic Syndrome - see HYPERSOMNOLENCE Nasopalpebral Reflex - see GLABELLAR TAP REFLEX Negative Myoclonus - see ASTERIXIS Negative Tremor - see ASTERIXIS Negativism Negativism is a motor sign of mental disorder, usually schizophrenia, consisting of the patient doing the opposite of what is asked and actively resisting efforts to persuade compliance. Movement of a limb in response to application of pressure despite the patient having been told to resist (mitgehen) is one element of negativism. The similarity of some of these features to gegen- halten suggests the possibility of frontal lobe dysfunction as the under- lying cause. Cross References Catatonia; Gegenhalten Neglect Neglect is a failure to orient toward, respond to, or report novel or meaningful stimuli. If failure to respond can be attributed to concur- rent sensory or motor deficits (e. Neglect of contralateral hemispace may also be called unilat- eral spatial neglect, hemi-inattention, or hemineglect. Lesser degrees of neglect may be manifest as extinction (double simultaneous stimula- tion). Motor neglect may be evident as hemiakinesia, hypokinesia, or motor impersistence. Neglect is commoner after right rather than left brain damage, usually of vascular origin. The angular gyrus and parahippocampal gyrus may be central to the development of visual neglect. Marked degrees of neglect may seriously hamper attempts at neurorehabili- tation. Reasons for variability in the reported rate of occurrence of unilateral spatial neglect after stroke. H ove: Psychology Press, 1996: 90-109 Alexia; Alloesthesia; Allokinesia; Asomatognosia; Extinction; Hemiakinesia; HypoKinesia; Impersistence Negro has two eponymous signs: ● Cogwheel (jerky) type of rigidity in basal ganglia disorders. Bell’s palsy; Facial paresis; Parkinsonism; Rigidity A neologism is a nonword approximating to a real word, produced in spontaneous speech; it is thought to result from an inability to organ- ize phonemes appropriately in the process of speech production. Hence, this is a type of literal or phonemic paraphasia encountered in aphasic syndromes, most usually those resulting from left superior temporal lobe damage (Wernicke type).