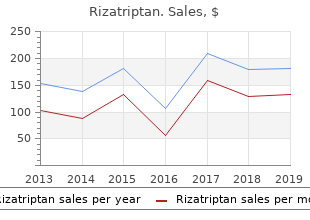

State University of New York College at Brockport. C. Thorek, MD: "Purchase online Rizatriptan cheap no RX - Cheap Rizatriptan online".
Optic neuritis and ischaemic neuropathy typically or signs in the neck discount 10 mg rizatriptan mastercard postoperative pain treatment guidelines, chest or hands pointing to the level cause early visual loss buy rizatriptan canada pain management treatment for spinal stenosis. Location of lesion Examples r Inferior ramus travels with superior ramus buy rizatriptan 10 mg with amex treatment for pain with shingles, but gives Sympathetic chain Carotid artery aneurysm or branches to inferior rectus and medial rectus muscles. It exits pos- wall of the cavernous sinus, then divides into: teriorly from the brainstem and winds around to the r Superior ramuswhich enters orbit via the lower part front, then passes in the lateral wall of the cavernous of superior orbital ssure within a tendinous ring. It exits from the brainstem and 1 V supplies the forehead, the upper eyelid and eyeball. Pain and temperature bres are also carried on the three divisions back to the trigeminal ganglion, but then dive Specic causes down into the medulla to the spinal nucleus of V which Particularly at risk from raised intracranial pressure or extends as far as the upper cervical cord. If touch is lost, but pain and temperature intact, Emerges as two roots (large sensory and small motor the lesion has to be in the pons or medulla. The Function motor nerve cell bodies are in the facial nerve nucleus in The motor components supply the muscles of mastica- the pons. Here the sensory nerve Management cellbodies cause a swelling called the geniculate ganglion If the patient is unable to close their eye completely, ar- and give off the nerve to stapedius and chorda tympani ticial tears should be used and the eye taped shut at (taste and lacrimation) before exiting the skull through night to prevent corneal ulceration. In cases that do not resolve tars- (frontalis) receives some innervation from each hemi- orrhaphy (suturing of upper to lower lid, laterally) may sphere, so that unilateral upper motor neurone lesions be necessary. Cosmetic surgery and/or reinnervation us- cause sparing of the forehead, whereas unilateral lower ing a lingual nerve transfer for example, can be used for motor neurone lesions cause forehead involvement. Function Prognosis Muscles of facial expression and taste of the anterior two A signicant proportion do not completely resolve and third of the tongue. The auditory bres arise from the cochlea and pass to the pontine auditory nucleus. The Clinical features vestibular nerves arise from the semicircular canals and The features of facial nerve palsy depend on the level pass to the vestibular nuclei in the pons, and the cerebel- of the lesion. Hyperacusis (hearing sounds louder than normal) sug- gests a lesion proximal to the stapedial branch. Function Hearing (cochlear nerve) and movement/position of head in space, for balance and head eye coordination Bell s palsy (vestibular nerve). As it is a lower motor neurone decit, the forehead is affected and the eye may not be able to close Clinical features completely. It usually begins to improve spontaneously Sensorineural deafness, tinnitus, vertigo, nystagmus. Anatomy Glossopharyngeal receives taste and common sensation This arises from the hypoglossal nucleus in the medulla, from the posterior third of the tongue, the oropharynx and is a motor nerve supplying the muscles of tongue viathe pharyngeal plexus, and the tonsillar fossa and soft except palatoglossus. It also carries autonomic innerva- Function tion to the heart, respiratory tract and gut. Specic causes Specic causes Stroke, bulbar palsy, polio, trauma and tuberculosis. Central causes include vascular lesions of the medulla, tumours, syringobulbia and motor neurone disease. Aneurysms and tumours in the posterior fossa and Clinical features meningitis may affect the nerves. The left recurrent la- Tongue deviates to side of lesion when patient is asked ryngeal nerve (a branch of the vagus) may be damaged to stick tongue out. In some cases there is a pure motor or pure sensory decit, but in most there is a combination of both. Damage to the peripheral nerves are Anatomy caused by a number of mechanisms, principally Spinal accessory branch arises from upper cervical cord r demyelination, segments and passes through the foramen magnum to r axonal loss, join the cranial accessory branch. They leave the skull r compression or traumatic sectioning of a nerve, separately through the jugular foramen. Function Cranial nerves join the pharyngeal plexus and supply the Mononeuropathies: Involvement of a single nerve. The spinal Traumatic peripheral nerve injuries may result from part supplies trapezius and sternocleidomastoid. Traumatic nerve damage may result in: r Neuropraxia, a transient loss of physiological function Specic causes with no loss in continuity and no degeneration. Clinical features r Axonotmesis, which follows more severe compression Weakness of lifting ipsilateral shoulder and turning head or traction damage, with Wallerian degeneration of against resistance towards the contralateral side. The nerve bun- dleisinterrupted, in-growth of brous tissue pre- vents re-innervation, so that surgical repair is needed Incidence if function is to be restored. Ideally, immediate repair Although rare (1 2 per 100,000 population per an- with end to end suture is undertaken with a reason- num), it is the commonest cause of acute accid paral- able prognosis. It affects all ages and both sexes nerve ends are marked with non-absorbable sutures equally. Aetiology/pathophysiology Any cause of mononeuritis multiplex may also present Immune mediated demyelination of peripheral nerves initially as a mononeuropathy. It is thought that antibodies to the infect- ropathy where two or more peripheral nerves are af- ing organism cross-react with components of myelin. If symmetrical In particular, recent infection with Campylobacter jejuni nerves are affected it may mimic a polyneuropathy. Clinical features Peripheral neuropathy: Asymmetrical disorder of pe- Patients complain of distal paraesthesiae and numbness ripheral nerves, usually distal more than proximal. The commonest causes are nerve involvement with difculty swallowing and respi- r Diabetes mellitus. Over the following weeks to months, the condi- r Vitamin B deciency (Thiamine (B )deciency in al- tion slowly improves. Other rare causes include uraemia; hypothyroidism; sys- temic diseases and vasculitis, e. Respiratory insufciency or aspiration risk (due to swal- Radiculopathy: Damage to one or more nerve roots or lowing difculties) may necessitate intubation and pos- anerve plexus. Traction injury during a difcult labour may they only fall late in respiratory failure. They are generally Clinical features r Erb s palsy (C5/6 lesions) with failure of abduction used for moderate to severe cases (i. Investigations Chest X-ray may show an apical lung lesion (Pancoast Brachial plexus injuries tumour)ora cervicalrib. The brachial plexus is formed from the nerve roots of C5 T1, which form into the medial, lateral and poste- Management rior cords. Pathophysiology Aetiology/pathophysiology The carpal tunnel is a tight space through which all the Mediannerveinjuriestendtooccurnearthewristorhigh tendons to the hand and the median nerve pass. Where the median nerve passes through cause of swelling is therefore likely to cause compres- the anterior cubital fossa under the biceps aponeurosis sion of the medial nerve. The condition is commonly into the forearm it is vulnerable to damage by forearm bilateral. It then passes under the exor retinaculum (through the carpal tunnel) into the hand low lesions are caused by com- Clinical features pression in carpal tunnel syndrome (see below), cuts to Tingling and numbness in the thumb, index nger and the wrist or carpal dislocation.
Informal reports from large groups of people (also known as crowd sourcing ) discount rizatriptan 10mg visa heel pain treatment exercises, when properly filtered and refined purchase rizatriptan online pain medication for dogs in heat, can produce data complementary to information from traditional sources discount rizatriptan 10 mg otc pain treatment on suboxone. One example is the use of information from the web to detect the spread of disease in a population. It also was able to track the progression and spread of H1N1 on a global scale when no particular public-health agency or health-care resource could produce that kind of a picture. The use of mobile phones also has tremendous potential, especially with developers building apps that engage patient populations. For example, a recent app called Outbreaks Near Me allows people to use their cell phones to learn about all the disease events in their neighborhood. People also can report back to the system, putting their own health information into the system. Many of the social networking sites built around medical conditions are patient specific and allow individuals to share unstructured information about health outcomes. Mining that information within proper ethical guidelines provides a novel opportunity to monitor health outcomes. For example, Google has mined de-identified search data to build a picture of flu trends. The advent of these inexpensive ways of collecting health information creates new opportunities to integrate information that will enhance the diagnosis and treatment of disease. Integrating Clinical Medicine and Basic Science Traditionally, a physician s office or clinic has had few direct connections with academic research laboratories. In this environment, patient-oriented research particularly if it involved studying patients or patient-derived samples with state-of-the-art scientific techniques and experimental designs required a major division of labor between the research and clinical settings. Typically, researchers have used informal referral networks to make contact with physicians caring for patients with diseases of special interest to the researchers. This approach often yielded descriptive and anecdotal results of uncertain relevance to larger (and more diverse) patient populations. Moreover, the patients who contributed are unlikely to remain connected to the 6 research process or be aware of outcomes. This research model is ill suited to long-term follow- up of patients since it was never designed for this purpose. Although remarkably successful in addressing its original goals of testing clearly defined hypotheses, this traditional approach to clinical research is poorly suited to answering current questions about human health that are often more open-ended and larger in scope than those typically addressed in the past. Based on committee experience and the input from multiple stakeholders during the course of this study, including the two-day workshop, the Committee 6 There are notable exceptions such as the Framingham Heart Study and Nurses Health study, which were designed from the outset to follow a cohort of patients over an extended period of time. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease 30 identified several reasons that current study designs are mismatched to current needs. Traditional designs: x Require very large sample sizes hence most studies are inevitably under-powered. As emphasized above, the number and complexity of questions inherent in genotype- phenotype correlations is virtually unbounded. Patients with particularly informative genotypes and phenotypes often difficult or impossible to recognize in advance will typically be rare. Identification and recruitment of such patients in sufficient numbers to acquire clinically actionable information about their diseases will be possible only if molecular and clinical information can be combined in huge patient cohorts. Indeed, the suite of obstacles that a young investigator must overcome to penetrate this system are a major disincentive for involvement in patient-oriented research. In addition, the many talented biomedical researchers who choose to focus their work on model organisms (such as flies, worms, and mice) have little opportunity to share insights or collaborate with clinical researchers. The current biomedical training system separates researchers and physicians from the earliest stages of their education and creates silos of specialized, but limited knowledge. The insular nature of the current biomedical system does not encourage interdisciplinary collaborations and has significant negative effects on training, study design, prioritization of research efforts, and translation of new research findings. Long-term follow-up was not required to conduct the first generation of genotype-phenotype studies. However, questions such as Do cystic fibrosis patients with particular genotypes do better over a period of decades with particular treatments? Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease 31 the results were generated, and whether the laboratory work was performed under protocols that permit results feedback. These limiting factors mean that most research results are not integrated into clinical care. Expert opinion on the duty to inform research participants of clinically relevant results vary widely. Indeed, many researchers are reluctant to contribute data to a common resource as it may expose them to questions about whether feedback to participants is necessary or desirable. In a sense, this challenge has parallels with the building of Europe s great cathedrals studies started by one generation will be completed by another, and plans will change over time as new techniques are developed and knowledge evolves. Many patients are already put on powerful drugs in their 40 s, 50 s, and 60 s that they will take for the rest of their lives. The very success of some cancer treatments is shifting attention from short-term survival to the long-term sequelae of treatment. For all these reasons, the era during which a genetic researcher simply needed a blood sample and a reliable diagnosis is passing. Outcomes research is also creating new opportunities for a close integration of medicine and data-intensive biology. Cost constraints on health-care services as well as an increasing appreciation of how often conventional medical wisdom is wrong has led to a growing outcomes-research enterprise that barely existed a few decades ago. The requirements of outcomes researchers for access to uniform medical records of large patient populations are remarkably similar to those of molecularly oriented researchers. Multiple Stakeholders Are Ready for Change The tremendous recent progress in genetics, molecular biology, and information technology has been projected to lead to novel therapeutics and improved health-care outcomes with reduced overall health-care costs. Clinical and basic researchers have learned that for their collective efforts to provide affordable improvements in health care, increased collaboration and coordination are required. Public-private collaborations are needed to combine longitudinal health outcomes data with new advances in technology and basic research. Such initiatives are essential to gain and apply the specific biological knowledge required to develop new approaches to treat and prevent disease. A dynamically evolving Knowledge Network of Disease would provide a framework in which a closer, more effective, relationship between clinical and basic researchers could thrive. Nowhere is the need for change more evident and urgent than in the pharmaceutical and biotechnology industries. Despite a massive increase in the amount of genomic and molecular information available over the past decade, the number of effective new therapies developed each year has remained stable, while the cost of developing each successful therapy has increased dramatically (Munos 2009). Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease 32 large number of novel drug targets, an inadequate biological understanding of these targets has resulted in an ever-increasing failure rate of expensive clinical trials (Arrowsmith 2011a,b). The pharmaceutical and biotechnology industries are now leading proponents for developing public-private collaborations and consortia in which longitudinal clinical outcomes data can be combined with new molecular technology to develop the deep biological understanding needed to re-define disease based on biological mechanisms. Given the time scale on which private entities must seek return on investment, there is an increased willingness to regard much of this information as pre-competitive. Hence, the information itself, and the costs of acquiring it, must be widely shared.
If possible proven 10mg rizatriptan pain treatment center new paltz, major decisions should be by consensus discount rizatriptan uk zona pain treatment, but different stakeholders may have different goals for documentation (or even oppose documentation) order rizatriptan 10 mg knee pain treatment bangalore. Carlini, Plants with Possible Psychoactive Effects Used by the Krah Indians, Brazil, 28 Rev Bras. Knowledge not already in written form should not be written down until a complete documentation strategy is in place. Depending on the knowledge in question, documentation can be costly and time-consuming. For example, traditional healers may need to be involved in documenting oral traditions or persons with language skills may be necessary to translate written texts. If documentation in electronic registries is desired, this requires computer equipment and technical expertise. For example, anthropologists from developed country universities may have valuable expertise in documenting traditional practices, but there may be concerns about transmitting knowledge outside of the community. The details of any proposed collaboration should be clearly agreed upon prior to the initiation of any substantive discussion, and should be governed by written contract rather than relying on informal agreements. However, just because information is publicly available does not mean it should not be documented. Because it is hard to know in advance what knowledge will prove useful in the future, it may be advisable to document as comprehensively as possible. A documentation plan should be created to detail exactly how data will be acquired and a timeline. If a product is being described, documentation should include all known names, variations, and both traditional and modern uses. If a process is being described, documentation should detail every step in the process, including all of the required materials and any information necessary to allow someone else to recreate the process. Documentation should also contain the name, location and contact information of stakeholders claiming ownership. Data is also significantly more accessible to researchers and patent examiners if provided in an electronic, searchable database. Finally, while full stakeholder involvement should be obtained as early as possible, it should be obtained no later than the beginning of the documentation. Written evidence of prior informed consent to documentation and future uses of traditional knowledge should be obtained. Once the documentation phase is ready to begin, the first step should be to comprehensively gather all existing sources of documentation. Based on existing documentation, stakeholders should evaluate where gaps in knowledge exist. For example, in addition to its modern role in treating peptic ulcer disease, the Chinese herbal formula Yi Wei Tang treats 43 217 yin deficiency from a traditional perspective. Terminology of this nature is useful to include in documentation, however it may not be easily comprehensible to outside parties. This includes efforts by the Indian government to document yoga practices in video. If external collaborators are involved in documentation efforts, these relationships should be carefully managed and the confidentiality of documentation maintained. A clear understanding of how documentation will be used should be in place prior to initiating documentation. It is reported that about 4,000 221 applications a year are submitted in this field domestically. An increasing number of these 222 patents are also entering the international patent system. Different ownership structures have different advantages and disadvantages, such as possible tax benefits or reduced personal liability. It is important to choose the most appropriate structure initially, for instance a corporation rather than a partnership, as changing forms of ownership later may be very difficult and costly. The specific structure of a business entity, for example how decisions will be made or how benefits will be distributed, may be shaped by contract, within the requirements of national law. Otherwise, and possibly even with a contract to the contrary, internal disputes may be governed by national law. In Germany, copyright 225 law permits alterations to a jointly created work only with the consent of all authors. However, a joint author may not unreasonably refuse consent to publish, exploit or alter a joint work. Its commercial value will be significantly lessened once knowledge becomes public. For example, a confidentiality clause could be written into research agreements to stipulate the recipient of such knowledge would be granted the right to use it in research and development but could not divulge the knowledge publicly. If documented knowledge is required for regulatory submissions, stakeholders should determine in advance whether that information will be kept confidential, and if so for how long. For example, to approve a foreign traditional medicine for marketing approval in Brazil, the Brazilian regulatory authority requires data to be submitted on clinical safety and efficacy. However, as a general matter, regulatory submissions may release data into the public domain. For information submitted to patent offices to be kept confidential, special licensing agreements may be necessary. The First Nation of Na-Cho Nyak Dun Government maintains holdings of documented traditional knowledge, and it serves as the primary contact for requests to access community traditional knowledge. The Government has established safeguards and information management systems that enable it to gather knowledge and 227 ensure appropriate and respectful use. The Government determines the sensitivity of traditional knowledge and accordingly restricts access. Knowledge is categorized as low sensitivity (information commonly known outside the community), medium sensitivity (information known only to those within the traditional community), and high sensitivity (spiritual information known only according to customary laws or information which might harm the community if it was released). Methods for restricting access include preventing reproductions of documentation or electronic exchange of information. The Government protects against unauthorized disclosure by limiting information access to authorized employees, specifying which additional persons may access information, and allowing users only to view information (prohibiting copying and distribution). Confidential data in electronic databases is further protected by allowing sign-on only by authorized staff, and by using passwords and read- only formatting. The European patent system does not limit evidence of prior art to printed publications, and includes everything made available to the public in writing or orally before the date of filing the patent application. If evidence of prior art is not found during the patent filing process and a patent is granted, the costs to have an existing patent invalidated may be significant. He has served as a consultant on health care financing and regulation, intellectual property and public health for international organizations, academic institutions and private enterprises including the World Health Organization and World Intellectual Property Organization.
The Committee believes that the best prospects for creating a similarly bright future for Patient 2 lies in achieving a similarly precise understanding of his disease by creating a Knowledge Network of Disease and an associated New Taxonomy cheap 10 mg rizatriptan with amex southern california pain treatment center agoura. Both these points suggested that we could best address our charge by framing the new-taxonomy challenge broadly purchase rizatriptan with american express knee pain treatment yoga. Many of the conclusions and recommendations could apply buy rizatriptan 10mg with amex canadian pain treatment guidelines, as well, to other challenges in translational research such as evaluating and refining existing treatments and developing new ones. However, disease classification is inextricably linked to all progress in medicine, and the Committee took the view that an ambitious initiative to address this challenge and particularly to modernize the discovery model for the needed research is an excellent place to start. The Committee thinks that the key to success lies in building new relationships that must span the whole spectrum of research and patient-care activities that comprise American medicine. Our recommendations seek to empower stakeholder communities by providing them with informational resources the Information Commons, the Knowledge Network, and the New Taxonomy itself that would transform the way they work and make decisions. At the core of the Committee s optimism is a conviction that dramatic advances in biological knowledge can be coupled more effectively than they are now to the goal of improving the health outcomes of individual patients. Biology has flourished in the 50+ years since the discovery of the molecular basis of inheritance. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease 65 Genome Project, genetics is in a golden age of discovery. Sequence similarity between genes studied in fruit flies and those studied in humans allows nearly instant recognition of the potential medical relevance of the most basic advances in biochemistry and cell biology. Increasingly, this process also works in reverse: unusual human patients call attention to molecules and biochemical pathways whose importance in basic biology had been overlooked or was otherwise inaccessible. Indeed, there are already many areas of basic biology in which human studies are leading the way to deep new insights into the way organisms work. For the simple reason that one can ask a research subject what she sees when looking at a pattern of light instead of having to develop a crude behavioral test to find out whether she sees anything at all we know far more about the molecular details of light reception in humans than we could ever have learned from studying mice. Particularly as biomedical research puts an increasing emphasis on unraveling the molecular underpinnings of behavior, the advantages of starting research studies with humans, rather than model organisms, are likely to grow. Experience tells us that translation of intensifying knowledge of basic biology into clinical advances is a daunting task. Furthermore, the Committee shares the sense that basic biology is at an inflection point in which there is every reason to expect increasing payoffs from the large investments in basic science that have brought us to this point. However, the grand challenge of coupling basic science more effectively to medicine will require a rethinking of current practices on a scale commensurate with the challenge. The Committee regards the initiative it proposes to develop the tripartite Information Commons, Knowledge Network, and New Taxonomy, as having the potential to rise to this level. Information technology is the key contributor to the technological convergence the Committee perceives. In medicine, information technology offers perhaps the best hope of increasing efficiency and improving our collective learning about what works and what does not. In a mere 20 years, people have made the transition from regarding most human knowledge as locked away in the dusty backrooms of research libraries to expecting it to be at their finger tips. Understandably, the public is losing patience with barriers to the sharing and dissemination of information. The social-networking phenomenon is a particularly dramatic illustration of changing attitudes toward information and associated blurring of the line between the public and private. The Committee recognizes that some aspects of the world we envision are more readily approachable than others. As emphasized throughout this report, there are many impediments to progress along the path we outline. That is the reason the Committee recommends pilot projects of increasing scope and scale as the vehicle for moving forward. Although we consider the creation of an improved classification of disease valuable in its own right, we do not recommend a crash program to pursue this goal in isolation from the broader reforms we emphasize. We regard smaller projects on the recommended path as preferable to larger, narrower initiatives that would distract attention and resources from these reforms. We think the impediments can best be overcome and the optimum design of the Information Commons, Knowledge Network, and the New Taxonomy best emerge in the context of pilot projects of increasing scope and scale. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease 66 Even some stakeholders in the health-care system who find the Committee s basic vision compelling may ask whether or not a special, organized effort is required to achieve the Committee s goals. In particular, some might argue that there are already enough examples many have been cited in this report in which data-intensive laboratory tests have such clear benefits for patients that the traditional system of test development and insurance reimbursement will allow a smooth transition to a new era of molecular medicine. Indeed, there is real risk of a backlash against premature claims of the efficacy of genomic medicine (Kolata 2011). The key to avoiding such a backlash is development of a robust system for discovering applications that have real clinical benefits and validating those claims through open processes. The Committee believes that expecting or pressuring payers in the health-care system to bear the costs of integrating data-intensive biology and medicine without clear evidence of the safety, efficacy, and economic feasibility of particular applications would fail indeed, such an effort could easily be counter-productive. On the other hand, as some of the scenarios sketched above indicate, the Committee believes that a well planned public investment in creating the system the Committee envisions would lead relatively quickly to robust public-private partnerships that would allow all stakeholders to build on early successes. Perhaps even more importantly, the Committee believes that its approach offers the most realistic available path to ultimate sustainability of precision medicine. Public investment in research can play an essential role in building a solid foundation for precision medicine, but it cannot sustain its dissemination: precision medicine will only become a routine aspect of health care when it pays its own way. To bring the discussion back to the Committee s core mission, we close by re- emphasizing our view toward disease taxonomy. Accurately and precisely defining a patient s condition does not assure effective treatment, but it is unequivocally the place to start. However, the Committee believes that implementation of its core recommendations would bring many new allies to the cause of improving this patient s health prospects and would equip these diverse players with powerful new tools and resources that are unlikely to emerge without an organized effort to create them. Medium-term exposure to traffic-related air pollution and markers of inflammation and endothelial function. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Physical activity and endometrial cancer in a population-based case-control study. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease 68 Biesecker, L. The ClinSeq project: Piloting large- scale genome sequencing for research in genomic medicine. The effect of altitude change on anemia treatment response in hemodialysis patients. Surveillance Sans Frontires: Internet-based emerging infectious disease intelligence and the HealthMap project. Rapid identification of myocardial infarction risk associated with diabetes medications using electronic medical records. Interactions between genetic variants and breast cancer risk factors in the breast and prostate cancer cohort consortium. Self-reported racial discrimination, response to unfair treatment, and coronary calcification in asymptomatic adults: The North Texas Healthy Heart study. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease Caspi, A. Genetic sensitivity to the environment: The case of the serotonin transporter gene and its implications for studying complex diseases and traits.
Buy cheap rizatriptan 10mg. Hip & Knee Warm-Up Stretches : Arthritis Pain Relief.